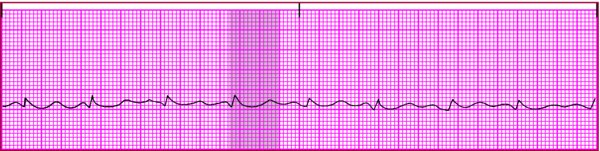
Prolonged from decreased calcium level (the key finding, as shown in shaded area on strip)
Other
Prolonged ST segment
What Causes It⬆⬇
Inadequate calcium intake due to diet deficient in green, leafy vegetables and dairy products
Excessive phosphorus intake (binds with calcium and prevents calcium absorption)
Pancreatitis (decreases ionized calcium)
Blood administration (the citrate solution in stored blood binds with calcium)
Neoplastic bone metastasis (decrease serum calcium levels)
Vitamin D deficiency due to inadequate intake or inadequate exposure to sunlight
Malabsorption of fats
Inadequate PTH levels (caused by removal of parathyroid glands)
Metabolic or respiratory alkalosis
Hypoalbuminemia (low albumin level)
What to Look for⬆⬇
Carpopedal spasm
Circumoral or digital paresthesia
Confusion
Hyperactive bowel sounds
Hyperreflexia
Intestinal cramping
Positive Chvostek sign
Positive Trousseau sign
Severe Hypocalcemia
Tetany
Seizures
Respiratory arrest
Death
How It's Treated⬆
Identify and manage the underlying cause.
Monitor serum calcium levels.
Administer IV calcium gluconate for severe symptoms. Keep calcium gluconate on hand for a patient with a positive Trousseau or Chvostek sign. Hypocalcemia may progress quickly to tetany, seizures, respiratory arrest, and death.
Replace calcium orally.
Identify and manage cardiac arrhythmias.
Instruct the patient to decrease phosphate intake.