AUTHOR: Shiva Kumar R. Mukkamalla, MD, MPH, FACP



Definition
Pernicious anemia (PA) is an autoimmune disease resulting from antibodies against gastric intrinsic factor and gastric parietal cells that results in vitamin B12 deficiency leading to megaloblastic anemia.
Synonyms
Megaloblastic anemia resulting from vitamin B12 deficiency
| ||||||||||||||||||||
Epidemiology & Demographics
- Increased incidence in females and older adults (40 to 70 yr)
- More frequent in patients of northern European ancestry
- Overall prevalence of undiagnosed PA after age 60 yr is 1.9%
- Prevalence is higher in women (2.7%), particularly in black women (4.3%)
- Associated with other autoimmune diseases (e.g., type 1 diabetes mellitus, Graves disease, Addison disease), along with possible Helicobacter pylori association
Physical Findings & Clinical Presentation12
- Mucosal pallor and/or glossitis (“beefy red tongue”)
- Angular cheilosis
- Mild jaundice (representative of intramedullary hemolysis of megaloblastic cells); “lemon yellow” skin due to pallor and jaundice
- Peripheral sensory neuropathy with paresthesias initially and absent reflexes in advanced disease
- Delirium or dementia
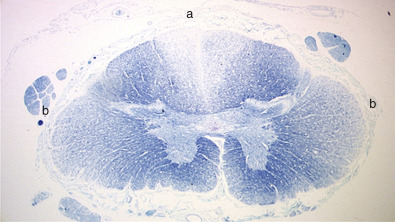
- Worsening weakness and possible subacute combined degeneration of spinal cord (Fig. E1)
- Loss of proprioception and an unsteady gait
- Gastrointestinal symptoms including anorexia, pyrosis, nausea, and vomiting
- Possible splenomegaly and mild hepatomegaly
Etiology34
- Parietal cell antibodies are present in >70% of patients, while intrinsic factor antibodies are noted in >50% of patients.
- Atrophic gastric mucosa (Fig. E2) with achlorhydria.
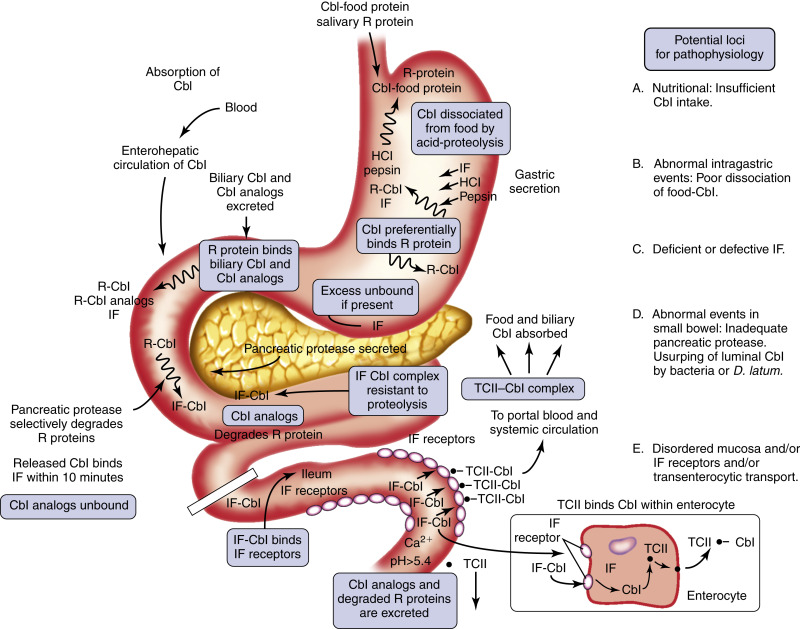
- Inborn errors of cobalamin-cofactor synthesis are rare. Fig. E3 illustrates the components and mechanism of cobalamin absorption. An etiopathophysiologic classification of cobalamin deficiency is described in Section II.
Figure E2 Histologic features of stomach in pernicious anemia compared with normal.
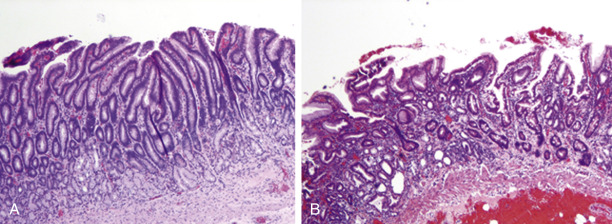
The normal gastric mucosa (A) is contrasted with that seen in pernicious anemia (B), in which there is atrophy of gastric glands, intestinal metaplasia with goblet cells, and loss of parietal cells (not visible at this magnification).
From Hoffman R et al: Hematology, basic principles and practice, ed 7, Philadelphia, 2018, Elsevier.