AUTHOR: Fred F. Ferri, MD




Ulcerative colitis (UC) is an idiopathic, remitting and relapsing, chronic inflammatory bowel disease (IBD) that starts in the rectum and extends proximally.
Inflammatory bowel disease (IBD)
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The incidence of UC is 9 to 12 cases/100,000 persons per yr in the U.S.; worldwide, the estimated incidence ranges from 1.2 to 20.3 cases/100,000 person-yr, and its prevalence ranges from 7.6 to 246.0/100,000 persons. It is most common between ages 15 and 40 yr, with a second peak between 50 and 80 yr. The disease affects men and women at similar rates. Infection with nontyphoid Salmonella or Campylobacter is associated with an 8 to 10 times higher risk of developing UC in the following year. Worldwide, UC is more common than Crohn disease.
The prevalence of UC is 7.6 to 246.0 cases/100,000 per yr. Higher prevalence in Ashkenazi Jewish descendants.
- Patients with UC often present with acute onset of bloody diarrhea accompanied by tenesmus, fever, and dehydration. At presentation 40% of adults have proctitis, 40% have left-sided colitis, and 20% have pancolitis. Diarrhea is not always present in UC patients with proctosigmoiditis and proctitis, and patients may have constipation.
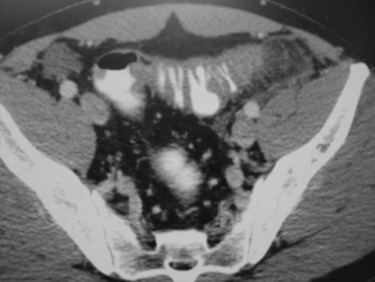
- Abdominal pain is not usually a prominent symptom. Abdominal distention and tenderness may indicate the presence of complications such as toxic megacolon.
- The onset of symptoms is typically acute and is generally followed by periods of spontaneous remission and frequent relapses.
- Fever, evidence of dehydration may be present during the acute flare-up.
- Evidence of extraintestinal manifestations may be present in nearly 25% of patients: Liver disease, sclerosing cholangitis, iritis, uveitis, episcleritis, arthritis, erythema nodosum, pyoderma gangrenosum, aphthous stomatitis. Box 1 summarizes common extraintestinal manifestations of UC.