AUTHOR: Glenn G. Fort, MD, MPH


Definition
Chronic rhinosinusitis (CRS) is an inflammatory condition that involves the paranasal passages and linings of the nasal passages that lasts 12 wk or longer despite medical therapy. It can be divided into three categories:
Epidemiology & Demographics
Incidence
CRS occurs in children and adults but is most frequently diagnosed in young and middle-aged adults.
Predominant Sex & Age
Some studies suggest women are more affected. In adults, the mean age of diagnosis was 39 yr.
Risk Factors
- Environmental or behavioral risk factors include:
- Host-associated risk factors: Allergic rhinitis, atopy, asthma, aspirin-exacerbated respiratory disease
- Innate immunodeficiencies: Cystic fibrosis
- Humoral immunodeficiencies: Common variable immunodeficiency, immunoglobulin A (IgA) or IgG subclass deficiencies, types of vasculitis (e.g., Churg-Strauss syndrome), and sarcoidosis
- Allergic fungal sinusitis
- Gastroesophageal reflux disease
- Odontogenic: Infectious agents from maxillary posterior teeth may breech into maxillary sinus
Physical Findings & Clinical Presentation
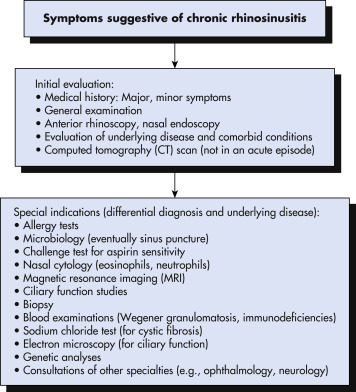
- CRS is diagnosed clinically with a physical examination and a detailed sinonasal history. There should be at least two out of the four cardinal symptoms for at least 12 consecutive wk:
- Objective evidence on physical examination using anterior rhinoscopy and nasal endoscopy includes mucopurulent drainage, edema, polyps in the middle meatus
- Radiographic evidence includes, preferably, computed tomography (CT) of sinuses.
- Features of specific subtypes:
- CRS without nasal polyposis: Most common type (60% to 65% of cases) with cardinal clinical symptoms
- CRS with nasal polyposis: Characterized with the presence of bilateral nasal polyps in the middle meatus, which are translucent masses composed of gelatinous inflammatory material, as well as cardinal clinical symptoms
- Allergic fungal rhinosinusitis:
Etiology
- Not fully understood but multifactorial involving host genetics and immunity, as well as environmental and infectious agents that produce chronic inflammation of the upper airways.
- Various cells, including fibroblasts, epithelial cells, endothelial cells, mast cells, eosinophils, antigen-presenting cells (dendritic cells), T cells, and B cells, have been shown to coordinate the immune inflammatory network underlying CRS, by the production of mediators such as cytokines, chemokines, eicosanoids, and antibodies.
- Microbiology: Organisms that may be involved in the pathogenesis of CRS include:
- Staphylococcus aureus: This is the most common bacterium and contributes to polyp formation. Methicillin-resistant S. aureus is isolated in 2% to 20% of patients with CRS.
- Coagulase-negative staphylococci: It is not always clear whether they are pathogens or colonizers.
- Pseudomonas aeruginosa: Occurs especially in patients with cystic fibrosis. Other gram-negative rods include Klebsiella pneumoniae, Proteus mirabilis, Enterobacter spp., and E. coli.
- Anaerobic bacteria include Peptostreptococcus, Fusobacterium, Prevotella spp., Porphyromonas spp.