AUTHOR: Joseph S. Kass, MD, JD, FAAN



Definition
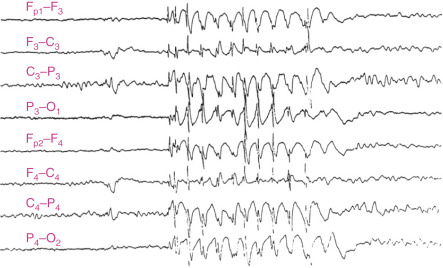
Absence seizures are a type of generalized seizure characterized by brief episodes of staring with impairment of consciousness (absence). They usually last no more than 20 to 30 sec. The onset and the end of the seizures are sudden. Patients are typically unaware of the seizure and resume the activity they were performing before the seizure. The electroencephalogram signature of absence seizures consists of a generalized 3-Hz spike and slow wave discharges.
Synonyms
| ||||||||
Epidemiology & Demographics
Predominant Sex and Age
More common in girls than in boys, absences typically begin between 4 and 10 yr and remit by age 201
Physical Findings & Clinical Presentation
- Patients with absence seizures usually have normal physical and neurologic examinations.
- During the seizures, the patients are unresponsive and can have motor phenomena (automatisms, eye blinks, mouth and hand movements).
- Absence seizures are not associated with post-ictal confusion.
- They may be triggered by hyperventilation associated with activity.
- Tonic clonic seizures are not usually a feature of this syndrome. If the patient also experiences tonic clonic seizures, other etiologies should be investigated, such as juvenile absence epilepsy, juvenile myoclonic epilepsy, complex partial seizures, etc.