AUTHOR: Fred F. Ferri, MD



Short bowel syndrome (SBS) is a malabsorption syndrome that results from extensive small intestinal resection or congenital causes (Table E1).
TABLE E1 Daily Stomal or Fecal Losses of Electrolytes, Minerals, and Trace Elements in Severe Short Bowel Syndrome∗
| Component | Amount Lost | ||
|---|---|---|---|
| Sodium | 90-100 mEq/L | ||
| Potassium | 10-20 mEq/L | ||
| Calcium | 772 (591-950) mg/day | ||
| Magnesium | 328 (263-419) mg/day | ||
| Iron | 11 (7-15) mg/day | ||
| Zinc | 12 (10-14) mg/day | ||
| Copper | 1.5 (0.5-2.3) mg/day |
∗For sodium and potassium, the average concentration per liter of stomal effluent is given. Values for minerals and trace elements are mean 24-h losses, with the range in parentheses.
From Feldman M et al: Sleisenger and Fordtran’s gastrointestinal and liver disease, ed 10, Philadelphia, 2016, Elsevier.
- Parallels Crohn disease (see “Crohn Disease” in Section I), which is the most common cause of the syndrome in adults.
- In children, two thirds of short bowels are related to congenital abnormalities (intestinal atresia, gastroschisis, volvulus, aganglionosis) and one third are related to necrotizing enterocolitis.
- Prevalence: 10,000 to 20,000 cases are estimated to exist in the U.S.
- Extensive bowel resection for treatment of the conditions mentioned previously (see “Epidemiology”). SBS typically does not occur until less than 200 cm of healthy small intestine remains. Risk for SBS is decreased if colon is intact.
- Congenital.
- Box E1 summarizes causes of short bowel syndrome.
BOX E1 Causes of Short Bowel Syndrome (SBS) and Intestinal Failure in Adults and Children
From Feldman M et al: Sleisenger and Fordtran’s gastrointestinal and liver disease, ed 10, Philadelphia, 2016, Elsevier.
The human intestine is 3 to 8 m in length. Removal of up to half of the small intestine produces no disruption in nutrient absorption, and most patients can maintain nutritional balance on oral feeding if they have more than 100 cm (3 ft) of jejunum. Similarly, 100 cm of intact jejunum can maintain a normal water, sodium, and potassium balance under normal circumstances. The presence of an intact colon can compensate for some small intestine loss.
Site-specific functions (Fig. E1):
- Calcium, magnesium, phosphorus, iron, and vitamins are absorbed in the duodenum and proximal jejunum.
- Vitamin B12 and bile acids are absorbed in the ileum. The resection of more than 60 cm of ileum results in vitamin B12 malabsorption. The loss of more than 100 cm results in fat malabsorption (from the loss of bile acids).
- The loss of gastrointestinal endocrine hormones can affect intestinal motility.
- Intestinal bacterial overgrowth may also occur, especially if the ileocecal valve is lost.
- Macronutrient requirements in patients with SBS are summarized in Table E2.
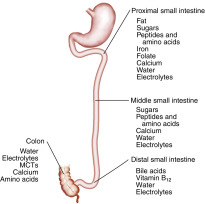
Macronutrients and micronutrients are absorbed predominantly in the proximal jejunum. Bile acids and vitamin B12 (cobalamin) are absorbed only in the ileum. Electrolytes and water are absorbed in both the small and large intestine. Medium-chain triglycerides (MCTs), calcium, and some amino acids can be absorbed in the colon.
From Feldman M et al: Sleisenger and Fordtran’s gastrointestinal and liver disease, ed 10, Philadelphia, 2016, Elsevier.
TABLE E2 Macronutrient Requirements in Patients With Short Bowel Syndrome
| Colon Present | Colon Absent | ||
|---|---|---|---|
| Carbohydrate | |||
| Complex carbohydrates/starches | Variable types | ||
| 30-35 kcal/kg per day | 30-35 kcal/kg per day | ||
| Soluble fiber | |||
| Fat | |||
| MCT/LCT | LCT | ||
| 20%-30% of caloric intake | 20%-30% of caloric intake | ||
| Protein | |||
| Intact protein | Intact protein | ||
| 1.0-1.5 g/kg per day | 1.0-1.5 g/kg per day | ||
LCT, Long-chain triglycerides; MCT, medium-chain triglycerides.
From Feldman M et al: Sleisenger and Fordtran’s gastrointestinal and liver disease, ed 10, Philadelphia, 2016, Elsevier.
∗Functional SBS can also occur in conditions associated with severe malabsorption and intact bowel length.