AUTHOR: Glenn G. Fort, MD, MPH

Definition
Yellow fever is a mosquito-borne infection, primarily of the liver, with systemic manifestations caused by the yellow fever virus (YFV), a flavivirus that infects the liver. The clinical spectrum ranges from asymptomatic infection to life-threatening disease with severity and mortality highest in the elderly.
Epidemiology & Demographics
Geographic Distribution
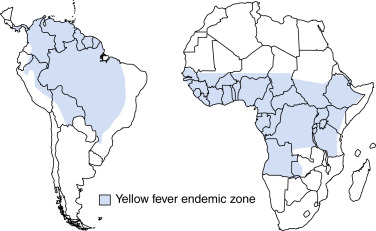
- South America and Africa, in countries between +15 and -15 degrees latitude (Fig. E1)
- The World Health Organization estimates there are more than 200,000 cases/yr with 30,000 deaths/yr. >90% of cases occur in Africa
- Outbreaks of yellow fever occurred in 2015 to 2018 in Angola and starting in 2016 in Brazil, which led that nation to recommend vaccination for the entire country instead of provinces that had traditionally had cases. In 2021, nine west African countries reported cases
Physical Findings & Clinical Presentation
Pathogenesis & Pathology
- Virus replication begins at site of mosquito bite, spreading to lymphatic channels and regional lymph nodes. Viremic spread to other organs, especially liver, spleen, and bone marrow.
- Shock and fatal illness result from direct damage to organs and vasoactive cytokines.
- Viral antigen found in hepatocytes, kidneys, and myocardium.
- Midzone necrosis of liver lobules primarily affected and is highly characteristic.
- Hemorrhages of mucosal surfaces of GI tract.


