AUTHOR: Fred F. Ferri, MD


Definition
Testicular torsion is a twisting of the spermatic cord leading to cessation of testicular blood flow, ischemia, and infarction if left untreated.
Physical Findings & Clinical Presentation
- Typical sequence is sudden onset of hemiscrotal pain, then swelling, nausea, and vomiting without fever or urinary symptoms.
- Physical examination may reveal a tender firm testis, high-riding testis, horizontal lie of testis, absent cremasteric reflex, and no pain with elevation of testis. Absence of the cremasteric reflex (stroking or pinching the medial thigh causing contraction of cremaster muscle and elevation of testis) is the most sensitive physical finding.
- Painless testicular swelling occurs in 10%.
- One out of three patients reports previous episodes of spontaneously remitting scrotal pain.
- In the neonate, testicular torsion should be presumed in patients with a painless, discolored hemiscrotal swelling.
- In rare cases, torsion may involve an undescended testicle. In such situations an empty hemiscrotum is palpated with a tender lump in the inguinal area.
Etiology
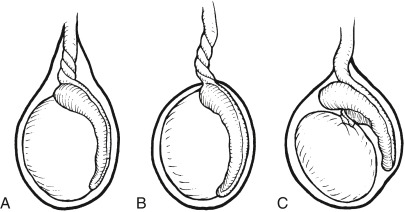
- There are three types of testicular torsion: Extravaginal, caused by nonadherence of the tunica vaginalis to the dartos layer; intravaginal torsion, caused by malrotation of the spermatic cord with the tunica vaginalis; and torsion of the testis below the epididymis (Fig. E1). Intravaginal torsion accounts for 90% of cases.
- Torsion usually occurs in the absence of any precipitating events. Trauma accounts for <10% of cases.