Why This Book Will Help You Be a Better Nurse: The Intersection of Nursing Care and Lab/Dx Testing
We hear every day from students and instructors that they want a laboratory and diagnostic test reference that will help them integrate laboratory and diagnostic test results into safe, compassionate, and effective nursing care. We revised the eleventh edition of the manual not only to be the comprehensive reference it was originally designed to be but also to provide improvements that more effectively answer that need. Our manual covers 22 different laboratory and diagnostic study types:
- Blood Studies, Clinical Chemistry
- Blood Studies, Hematology
- Blood Studies, Hemostasis (Coagulation)
- Blood Studies, Immunohematology (Blood Banking)
- Blood Studies, Immunology
- Body Fluid Analysis Studies
- Computed Tomography Studies
- Electrophysiological Studies
- Endoscopic Studies
- Fecal Analysis Studies
- Manometric Studies
- Magnetic Resonance Imaging Studies
- Nuclear Medicine Studies
- Pulmonary Function Studies
- Radiological Studies Contrast/Special
- Radiological Studies Plain
- Sensory Studies: Auditory
- Sensory Studies: Ocular
- Skin Tests
- Tissue and Cell Microscopy Studies: Histology/Cytology
- Ultrasound Studies
- Urine Studies
Lab and diagnostic testing is usually applied from the general and least invasive studies to more specific and invasive studies. A small group of studies in this manual have been identified as Core Lab and Core Diagnostic Studies, designated with the following tabs in the entry title: . The designation is meant to assist the reader in sorting and prioritizing the basic “always need to know” laboratory studies from the hundreds of other valuable studies found in the manual. Normal, abnormal, or various combinations of core study results can indicate that all is well, reveal a problem that requires further investigation with additional testing, signal a positive response to treatment, or suggest that the health status is as expected for the associated situation and time frame. The Index includes entries for core laboratory studies and core diagnostic studies as follows, for quick reference.
Core Lab Studies
- Alanine Aminotransferase
- Albumin and Albumin/Globulin Ratio
- Alkaline Phosphatase and Isoenzymes
- Amniotic Fluid Analysis and L/S Ratio
- Aspartate Aminotransferase
- Bilirubin and Bilirubin Fractions
- Blood Gases
- Blood Typing, Antibody Screen, and Crossmatch
- Calcium, Blood, Total and Ionized and Urine
- Cholesterol, Total and Fractions
- Creatinine, Blood and Estimated Glomerular Filtration Rate (eGFR)
- Fecal Analysis
- Glucose
- Hemoglobin A1C
- Hemoglobin and Hematocrit
- Human Chorionic Gonadotropin
- Human Immunodeficiency Virus Testing
- Newborn Screening
- Papanicolaou Smear
- Partial Thromboplastin Time, Activated
- Platelet Count and Tests of Platelet Function
- Potassium, Blood and Urine
- Prothrombin Time and International Normalized Ratio
- Sodium, Blood and Urine
- Troponins I and T
- Urea Nitrogen, Blood and Urine
- Urinalysis
- White Blood Cell Count, Blood Smear and Differential
Core Diagnostic Studies
- Audiometry, Hearing Loss
- Bone Mineral Densitometry
- Bone X-Ray
- Chest X-Ray
- Colonoscopy
- Computed Tomography, Various Sites
- Echocardiography
- Echocardiography, Transesophageal
- Electrocardiogram
- Electroencephalography
- Fetoscopy
- Gastroesophageal Reflux Scan
- Holter Monitor
- Hysterosalpingography
- Liver Scan
- Magnetic Resonance Imaging, Various Sites
- Mammography
- Positron Emission Tomography, Various Sites
- Pulmonary Function Studies
- Pulse Oximetry
- Slit-Lamp Biomicroscopy
- Stress Testing: Exercise and Pharmacological
- Ultrasound, Biophysical Profile, Obstetric
- Ultrasound Studies, Various Sites
- Venography, Lower Extremity Studies
WHAT IS NEW IN THE 11TH EDITION?
We continue to provide a portable product while making sure that each study stands on its own without repeating general information shared by most studies.
Tables of potential nursing problems have been created for or revised in all of the core laboratory and core diagnostic studies.
We address more than 700 study findings in 300 individual entries. We added more than 20 new substudy findings to entries already presented in the manual:
- Albumin, urine random (see Albumin, Urine and Albumin/Creatinine Ratio [acr])
- Proteinase 3 antibodies (see Antineutrophil Cytoplasmic Antibody [P-ANCA, C-Anca])
- Prosigna (see Biopsy, Breast)
- Genetic variants associated with Lynch syndrome (see Cancer Markers)
- Ceramides: Cer16:0, Cer18:0, Cer24:1 associated with cardiovascular disease and insulin resistance (see Cholesterol, Total and Fractions)
- Group B streptococcus antigen rapid urine screen and group B streptococcus antigen anal/genital testing (see Culture, Bacterial Various Sites, Anal/Genital, Urine)
- Calprotectin (see Fecal Analysis)
- Screening tests for colon cancer (see Fecal Analysis)
- Optical coherence tomography (see Fluorescein Angiography and Optical Coherence Tomography)
- Insulin-like growth factor 1 (IGF1) and insulin-like growth factor binding protein-3 (IGFBP-3) (see Growth Hormone, Stimulation and Suppression Tests)
- HBSAg (quantitative), HBcAg (quantitative), anti-HBS (quantitative), HBV DNA (quantitative), HBV genotyping, HCV RNA (quantitative), HCV genotype, HCV genotype antiviral drug resistance, HDVAg (qualitative), HEV DNA (quantitative) (see Hepatitis Testing)
- Hydrogen breath test and stool test for lactose intolerance (see Lactose Tolerance Test)
- EBV antibody to early antigen D, EBV antibody to nuclear antigen, EBV antibody to viral capsid antigen (IgM), EBV antibody to viral capsid antigen (IgG) (see Mononucleosis Testing)
- RBC Band 3 protein reduction (see Osmotic Fragility)
- PI-linked antigen (see Paroxysmal Nocturnal Hemoglobinuria Testing)
- Blood, CSF, and imaging tests for Alzheimer and Parkinson disease (see Positron Emission Tomography, Various Sites (Brain))
- Dopamine transporter scan (DaT scan) and Syn-One® skin biopsy for Parkinson disease (see Positron Emission Tomography, Various Sites [brain])
- Aldosterone-renin ratio (see Renin)
- 14-3-3 eta protein (see Rheumatoid Factor)
- Genetic testing (karyotype for CFTR, AZF deletions) (see Semen Analysis)
- Optomap and CMS examination elements (see Slit-Lamp Biomicroscopy)
- Toe brachial index (see Ultrasound, Arterial Doppler, Lower and Upper Extremity Studies)
- Allen test (see Appendix A: Patient Preparation and Specimen Collection)
Renamed studies:
- Glucose (formerly Glucose, 1-5 Anhydroglucitol, and Fructosamine)
- Paroxysmal nocturnal hemoglobinuria testing includes acid hemolysis test and PI-linked antigen (formerly Ham test for paroxysmal nocturnal hemoglobinuria testing)
- Prenatal Screening Tests (formerly Maternal Markers)
Other new changes to the manual’s content include the following:
- Numerous revisions and updates:
- Evolving information regarding the identification of risk factors related to family cancer (also known as inherited family cancer); father-to-daughter X-linked transmission of ovarian cancer
- Updated surveillance guidelines regarding recurrence in breast cancer
- Updated guidelines for blood pressure in people with diabetes (cardiac catheterization, cholesterol, stress testing)
- Updated guidelines for direct LDL normal values, by age group
- Updated guidelines for colon cancer screening (colonoscopy)
- Updated guidelines for breast cancer screening (mammography)
- Addition of some disease-specific dietary recommendations (e.g., Antigliadin antibody).
- Addition of artificial intelligence technology in ophthalmic studies (fluorescein angiography and fundus photography)
- Retirement of obsolete tests:
- Aldolase (see CK, ALT, and AST as markers of muscle or liver damage)
- Bleeding Time (see Platelet Count and Tests of Platelet Function)
- Clot Retraction (see Platelet Count and Tests of Platelet Function)
- Gastric Analysis (see Esophageal Manometry)
- Lactate Dehydrogenase and Isoenzymes (see Troponins, Creatine Kinase and Isoenzymes)
- Leukocyte Alkaline Phosphatase (see Cancer Markers—added Bcr/Abl)
- Myoglobin (see Troponins, Creatine Kinase and Isoenzymes)
- Index:
- The index has been simplified and shortened.
- Entries for all main study titles are in BOLD font to make them easier to identify.
- Entries for subtests are listed alphabetically as well as under the corresponding main study title.
- Entries for the retired studies remain in the index and are accompanied by page references to the more relevant, commonly requested studies.
- New entries were created to list the core lab studies, blood studies, body fluid studies/substudies, diagnostic studies, and critical findings summary tables.
- Appendices. Appendices A, B, and C remain in print; Appendices D, E, and F have been moved to FADavis.com.
- Appendix A: Patient Preparation and Specimen Collection
- Appendix B: Laboratory Critical Findings
- Appendix C: Diagnostic Critical Findings
- Appendix D: Skin Assessment for Infection, Hematoma, and Pressure Damage
- Appendix E: Current Trends in Health Care UPDATED: Laboratory and Diagnostic studies that involve images and large data sets are the types of studies that more commonly utilize variations of artificial intelligence; further discussed in the updated Appendix E.
- Appendix F: The Human Microbiome: Patient Care Considerations for Nurses
WHAT WE KEPT FROM PREVIOUS EDITIONS
- FOR INSTRUCTORS: Our instructor resources provide 13 system-based case studies in PowerPoint format that include Next-Generation NCLEX® style questions. These case studies will help students think critically about how laboratory studies and diagnostic testing play an important role in clinical judgment and are accompanied by active classroom lesson plans. Adopters can find these resources in the Instructor section on FADavis.com.
- FOR INSTRUCTORS AND STUDENTS: We reviewed the student checklist located in the back of the book. The checklist condenses the main nurse-centered information in one place, organized by phase (pretest, intratest, and posttest).
- We present a clinical judgment statement at the end of each study. Consider them concise, inspirational Words of Wisdom—our WOW factor. Nursing is a complex profession. Clinical judgment is a skill that grows over time as the nurse explores and links actions taken to results achieved. We all strive to control our work environment. However, when that environment is centered on a living, breathing human being, control can be an illusion. The clinical judgment statements are intended to help student and novice nurses recognize the value of nursing wisdom in relieving physical pain and emotional distress. Physical pain is not the only way a patient can suffer. The long-range effects of a diagnosis can change a patient’s life at every level. Nurses must always strive to be in tune with not just the physical pain but the emotional and spiritual pain that patients may be experiencing. In the end, the most we can do is to provide information, emotional and spiritual support, and clinical expertise in assisting the patient to meet their medical challenges. Collaboration with others, including the family and patients themselves, is the only path to success. Development of strong clinical judgment skills helps us center our care on our patients’ wants and needs with consideration of the patients’ individual circumstances.
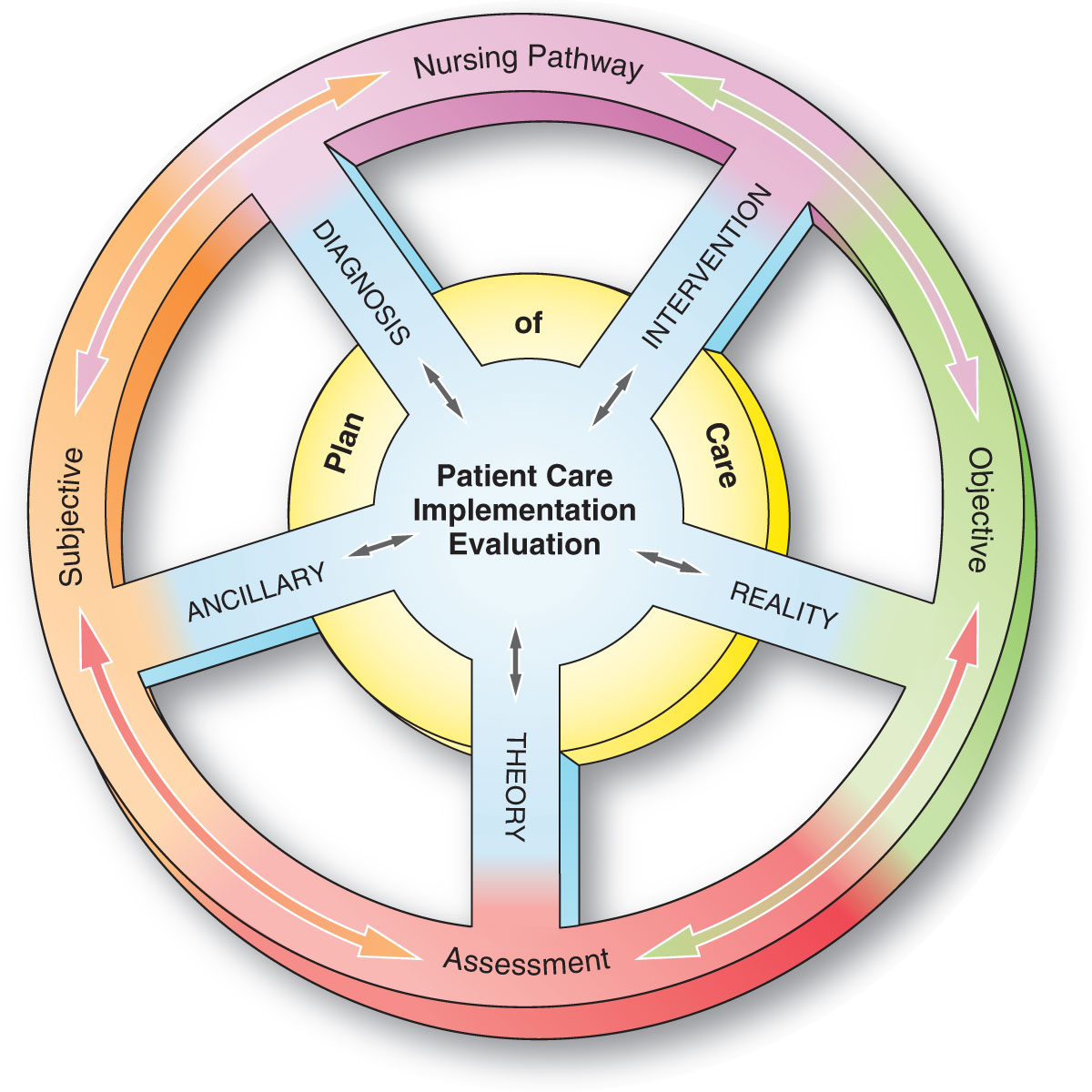
- Integration of clinical judgment: A decision-making model and corresponding icon for Clinical Judgment is included in the Nursing Implications section. This helps the reader integrate the nursing process and clinical judgment at the point of care. One of the greatest challenges of becoming a nurse is in understanding how to use the nursing process in a practical way. The nursing process (assessment, diagnosis/analysis, planning, implementation, evaluation) is the gold standard by which generations of nurses have approached patient care. Over time, other terms have been added to enhance the problem-solving process. Terms such as critical thinking (logical interpretation of raw data), clinical reasoning (use of assessment data to identify a nursing problem/diagnosis and plan of care), and clinical judgment (combination of data analysis and intuitive thought) are additional concepts now imbedded within the nursing process purview. The concept of clinical judgment is a more recently integrated concept embracing both critical thinking and clinical reasoning to help students/instructors/nurses focus on patient management and related teaching/learning needs. Clinical judgment is a blend of factual and intuitive thought focused on specific patient problems as we ask the questions, “What should I do in this situation, and why?” Clinical judgment expands, grows, and improves exponentially with on-the-job experience. Information used to inform clinical judgment is gathered through the application of nursing process. In weaving the concept of clinical judgment throughout the nursing process, it is easy to see how it is used across the spectrum of patient care. We use clinical judgment (recognize cues) and nursing process (assessment) to weed out data that are pertinent to the issue at hand from that which are not. We use clinical judgment (analyze cues, prioritize hypotheses) and nursing process (diagnosis/analysis) to identify patient problems. We use clinical judgment (generate solutions) and nursing process (planning) to sort through available treatment options and choose those that will promote the best outcome. Clinical judgment (take action) and nursing process (implementation) put the plan into action. Clinical judgment (evaluate outcome) and nursing process (evaluation) decide if the plan worked or not and what revisions need to be made to try again. The decision-making model (Figure FM–1) is a tool we constructed to help students see the process of thinking like a nurse with the application of nursing process and clinical judgment. This type of decision making should always be considered within the context of the individual patient’s clinical situation.
- Organization of study content: An efficient design is used that places the “need to know” information at the beginning of each study.
- Information about patient preparation remains at the top of each study.
- Information about critical findings immediately follows the section on Normal Findings. Critical Findings sections include the following:
- A simple statement that reinforces the role of the nurse in providing timely notification and documentation of critical values
- Applicable adult, pediatric, and neonatal values
- Values in conventional and SI units
- Potential interventions
The following are highlights of unique content that we kept and updated:
- Indications: Examples of step-by-step interpretations of arterial blood gas results for the four main types of acid-base imbalance (see study titled “Blood Gases”).
- Nursing Implications subheadings were changed to reflect the active application of Nursing Process.
- Potential Nursing Problems: Assessment & Diagnosis/Analysis
- Before the Study: Planning and Implementation
- After the Study: Implementation and Evaluation
- Follow-Up and Desired Outcomes
- Teaching the Patient What to Expect: The explanation of the procedural portion of each study is explained in patient-friendly language and provides the information a nurse would need to
- Describe the procedure’s common use; why the health-care provider has ordered the test
- Describe how and where the procedure is conducted
- Answer questions, and provide reassurance
- Evidence-based practice is reflected throughout in
- Suggestions for patient teaching that reflect changes in standards of care, particularly with respect to current guidelines
- The most current Centers for Disease Control and Prevention guidelines for infections such as hepatitis, HIV, HPV, Lyme disease, syphilis, tuberculosis, and a number of commonly encountered bacterial and viral infections
- The most current guidelines for assessment of atherosclerotic cardiovascular disease, blood product safety, breast cancer, colon cancer, diabetes, heart failure, infectious diseases, lead poisoning, lung cancer, newborn screening, osteoporosis, prenatal testing, prostate cancer, rheumatoid arthritis, sepsis, skin cancer, systemic lupus erythematosus, vaccination recommendations
- Best practices for preventing surgical site infections
- Best practices for addressing the need to obtain informed/written consent
- We address real-life, potentially controversial topics using examples of situations nurses will encounter. A few examples include
- Child or elder abuse (Indications section of “Bone X-ray”)
- Childhood and adult vaccinations (Follow-up and Desired Outcomes section of “Antinuclear Antibody, Anti-DNA Antibody, Anticentromere Antibody, Antiextractable Nuclear Antigen Antibody, Anti-Jo Antibody, and Antiscleroderma Antibody”; Overview section of “Varicella Testing”; Teaching the Patient What to Expect (Potential Nursing Actions) and Treatment Considerations section of “Viral Testing”)
- Patients considering genetic testing (sections throughout “Cancer Markers” and “Prenatal Screening Tests”)
- Patients who have been sexually assaulted (Treatment Considerations and Clinical Judgement sections of “Hepatitis Testing,” “Human Immunodeficiency Virus Testing,” “Viral Testing”)
- We cover disease-related nutritional recommendations and cancer screening guidelines but have limited the detailed information in closely related studies to a study commonly used to diagnose the condition. There are now six main studies with detailed guidelines (atherosclerotic cardiovascular disease [ASCVD], diabetes, breast CA, prostate CA, colon CA, cervical CA). We refer readers to the relevant main study for these guidelines.
- Repetitive content has been moved to Appendix A from the diagnostic testing subsections: avoiding complications, interfering factors/contraindications, teaching the patient what to expect, and treatment considerations.