Treatment Options for the Management of Parkinson's Disease (PD) 
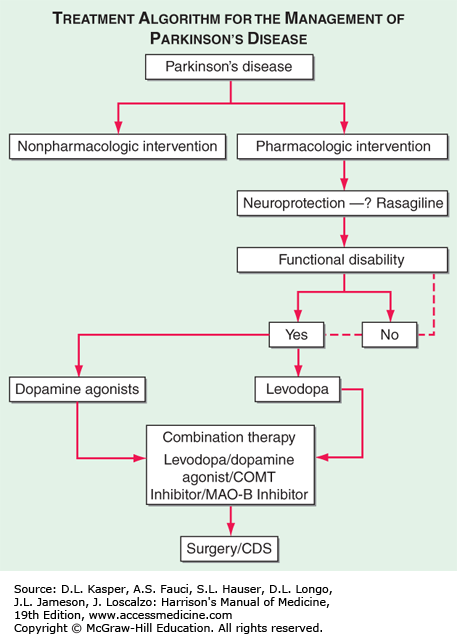
Treatment options for the management of Parkinson's disease (PD). Decision points include: (1) Introduction of a neuroprotective therapy: No drug has been established to have or is currently approved for neuroprotection or disease modification, but there are several agents that have this potential based on laboratory and preliminary clinical studies (e.g., rasagiline 1 mg/d, coenzyme Q10 1200 mg/d, the dopamine agonists ropinirole, and pramipexole). (2) When to initiate symptomatic therapy: There is a trend toward initiating therapy at the time of diagnosis or early in the course of the disease because pts may have some disability even at an early stage, and there is the possibility that early treatment may preserve beneficial compensatory mechanisms; however, some experts recommend waiting until there is functional disability before initiating therapy. (3) What therapy to initiate: Many experts favor starting with a monoamine oxidase type B (MAO-B) inhibitor in mildly affected pts because of the good safety profile of the drug and the potential for a disease-modifying effect; dopamine agonists for younger pts with functionally significant disability to reduce the risk of motor complications; and levodopa for pts with more advanced disease, the elderly, or those with cognitive impairment. Recent studies suggest the early employment of polypharmacy using low doses of multiple drugs to avoid side effects associated with high doses of any one agent. (4) Management of motor complications: Motor complications are typically approached with combination therapy to try and reduce dyskinesia and enhance the “on” time. When medical therapies cannot provide satisfactory control, surgical therapies such as DBS or continuous infusion of levodopa/carbidopa intestinal gel can be considered. (5) Nonpharmacologic approaches: Interventions such as exercise, education, and support should be considered throughout the course of the disease. CDS, continuous dopaminergic stimulation; COMT, catechol-O-methyltransferase. (Adapted from C Olanow et al: Neurology 72:S1, 2009.)