Information ⬇
Figure 44-1 Exposure to hazardous drugs and protection strategies.
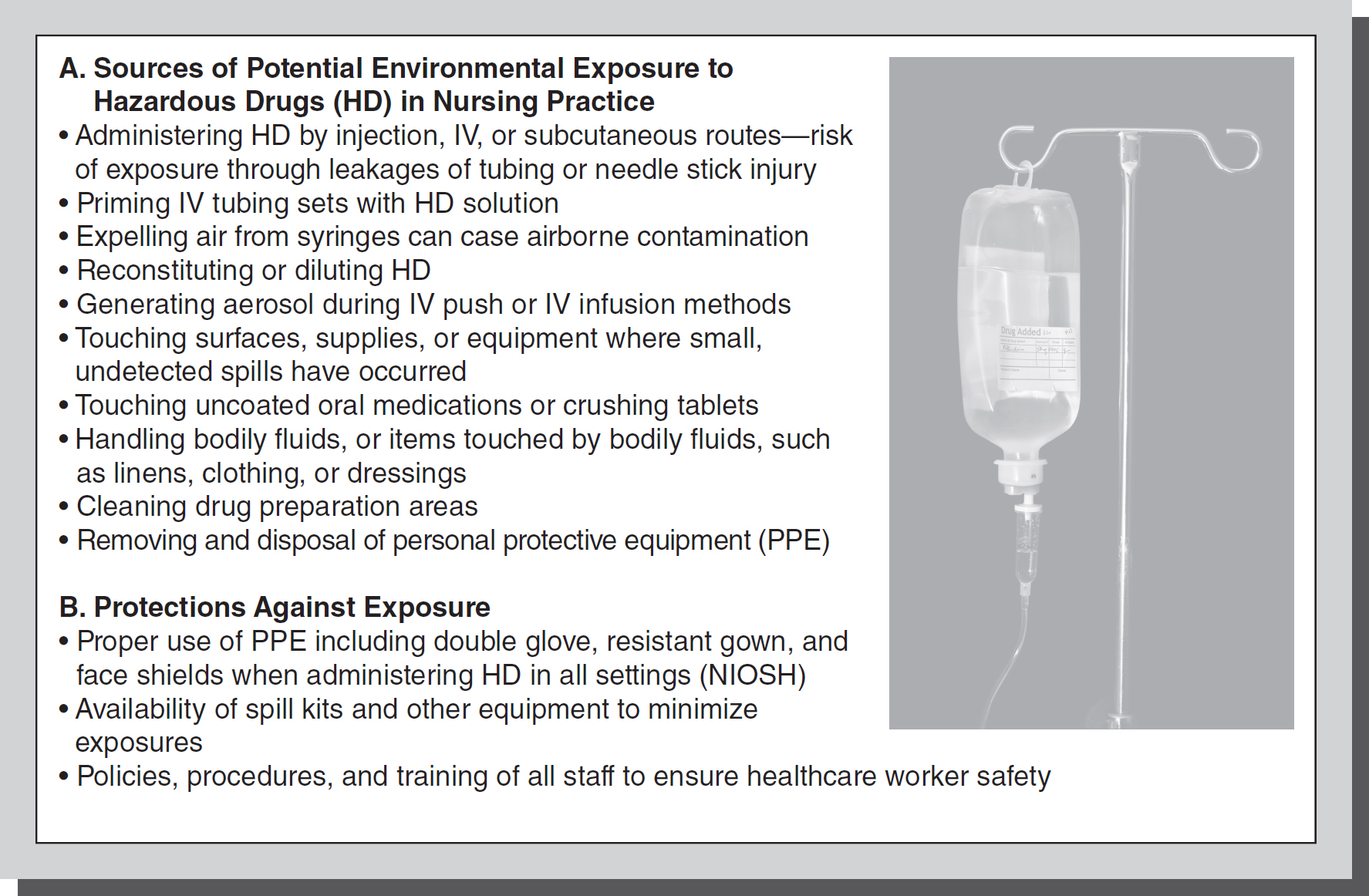
© Jones & Bartlett Learning; © Lim Yong Hian/Shutterstock
Creating safe work environments in healthcare institutions and agencies has become a priority. Exposure to chemicals, drugs, unsafe equipment, environmental hazards, and unsafe working conditions presents risks for nurses and other healthcare workers. This has prompted regulatory, governmental, and professional organizations to formulate recommendations, policies, laws, and enforcement procedures to protect workers. The American
Nurses Association (ANA) “Nursing Scope and Standards of Practice” (2021) states that the registered nurse practices in a manner that advances environmental health and safety. Additionally, there has been noteworthy interest in creating a more “green” emphasis in healthcare delivery. The effects of climate change have also received attention from nurses and have been recognized as affecting health and safety. Nurses continue to take an active role in these environmentally conscious initiatives and programs.
Occupational Health and Safety Administration (OHSA) ⬆ ⬇
OSHA's mission is to assure the safety and health of workers through setting and enforcing standards; providing training, outreach, and education; establishing partnerships; and encouraging continual improvement in workplace safety and health. The Occupational Health and Safety Act of 1970 established the processes and enforcement structures for workplace safety. The driving forces for the legislation were that workplace illnesses and injuries resulted in lost production, medical expenses, wage losses, and disability payments that were significantly impacting businesses in the nation. This is in addition to the personal and human resource loss related to injury of individuals. OSHA's aims include reducing the number of occupational safety and health hazards, specifying rights and responsibilities of employers and employees in the processes, setting standards that would then be enforced, exploring relationships between environmental conditions and the development of illnesses, and providing training programs for persons specializing in this field. As part of the enforcement of standards, unannounced periodic inspections are made to worksites, and reporting procedures by agencies are required. Employers and employees must both follow rules, regulations, and health standards set by OSHA. For example, there are regulations for personal protective equipment (PPE) to be worn by healthcare workers when performing certain tasks. An example of PPE use is that gloves must be worn as a standard precaution when handling objects that are contaminated with blood or bodily fluids of patients. Despite shortages of some PPE during the COVID pandemic, OSHA regulations have remained in place. However, certain regulations have been altered or relaxed in some instances due to emergency measures and shortages of equipment that have emerged. Professional groups and staff continue to advocate for safe work environments during such challenging circumstances and emergency situations.
Another requirement for employers (if they have more than 11 employees) is that they must keep records of all occupational injuries and illnesses. Employers must also provide education for employees about the health and safety of the jobs they are performing, including posting some educational material in plain sight at the workplace. They must also provide the PPE necessary for employees to perform their jobs, such as gowns, gloves, and facemasks that may be required to care for patients in isolation. Employees must notify their employers of any hazardous working condition, and may file a complaint with OSHA if there is no employer response. Employers may be liable for negligence to employees for exposure to dangerous conditions, especially if the conditions are in violation of OSHA standards.
The National Institute of Occupational Safety and Health (NIOSH) ⬆ ⬇
The NIOSH is a federal agency of the Centers for Disease Control and Prevention (CDC) that is a repository of information on safety and health information for healthcare workers and others. For example, the NIOSH sets weight limits for safe lifting that are recommended for ergonomic safety, including a limit of 35 pounds for women, and a 55-pound limit for men. The agency also publishes standards and recommendations such as those for safe handling and administration of antineoplastic agents and other hazardous drugs (HD).
Ergonomic Safety and Safe Patient Handling Campaigns ⬆ ⬇
Due to the nature of their work, nurses are subject to a high rate of exposure to musculoskeletal and other occupational injuries, including low-back, neck, and shoulder injuries. The physical nature of the work of lifting, moving, positioning, and attending to patient's needs puts nurses at risk. This risk for injury increases when moving and assisting patients who have a higher body weight. According to a recent study by Tucker and Parker (2022), 10-year weight-gain patterns have increased in the general U.S. population. These factors have led to recent initiatives by the American Nurses Association (ANA) and others to promote safer patient movement and handling. These proactive, evidenced-based programs have resulted in “no lift” policies in some institutions. Instead of staff lifting patients, equipment is used in its place. Algorithms have been developed to promote recommended practices in lifting, moving, and transferring patients. In 2003, the ANA established the “Handle with Care” campaign that advocates for change from traditional manual lifting to an assistive device approach. The ANA has a current “Handle with Care” initiative that includes an informative “Safe Patient Handling and Mobility” (SPHM) pamphlet (ANA, 2015). Results from an (ANA) survey of nurses outlined the scope of this problem. More than any other work-related injury or illness, musculoskeletal disorders (MSDs) are responsible for lost work time, long-term medical care, and permanent disability among healthcare workers. Sixty-two percent reported developing a disabling MSD as a top health and safety concern. Fifty-six percent say they have experienced pain from MSDs that was exacerbated by their job, and 80 percent reported pain from MSDs but continued to work despite experiencing frequent pain (ANA, 2015).
Noble and Sweeney (2018) conducted a study to identify barriers to the use of assistive devices for lifting and moving patients by nurses. They found that nurses' perceived staffing levels and workload, availability and accessibility of equipment, and emergent patient needs as the leading time constraints contributing to the lack of assistive device use in patient handling and mobility. Accessibility of equipment was significant because the majority of nurses reported that equipment was too far away and too difficult to retrieve or remove from storage. These authors note that improvements are needed within SPHM programs to reduce these barriers and to promote a safer workplace to prevent workplace-related musculoskeletal injuries (Noble and Sweeney, 2018).
Workplace injuries have impacts not only on the individual but also on the organization in terms of employee absence, productivity, and worker's compensation. Some individuals may need to be transferred to other areas of practice or may leave the profession because of injuries. Worker's compensation claims can be a significant cost to employers. In one case, an RN sought worker's compensation for an injury to her knee from helping another nurse move a patient. The Labor and Industrial Relations Commission denied the compensation, because it determined that Nurse Tillotson had preexisting arthritis in her knee and that she required a knee replacement primarily because of this and not her torn lateral meniscus from the workplace injury. However, the Missouri Court of Appeals reversed this finding and found that in order to cure and relieve the injury, the total knee replacement was reasonably required, and therefore compensable under the worker's compensation claim. She was awarded compensation for the cost of the total knee replacement, the period of disability that followed when she could not work as an RN, and permanent partial disability from the injury (Tillotson v. St. Joseph Medical Center, 2011).
Occupational Exposure to Hazardous Drugs and Substances ⬆ ⬇
Nurses have long been concerned about occupational exposures to hazardous drugs and products in the workplace. See Figure 44-1. Cytotoxic and genotoxic risks have been identified since the 1970s for drug exposures to antineoplastic agents for healthcare workers who handle these agents. In response, NIOSH and OSHA have developed guidelines to protect nursing staff against antineoplastic drug exposure, including the following:
- The use of protective gloves and gowns when preparing, handling, administering, or handling waste or excreta containing antineoplastic agents
- Training for all employees who are involved in their use upon start of employment
- Continuing education on how to handle hazardous drugs (Stover & Achutan, 2011, p. D1)
NIOSH has compiled a list of hazardous drugs (including chemotherapy and antineoplastic agents), which is updated periodically and is available on its website (http://www.niosh.gov). The agency uses recommendations from the Food and Drug Administration (FDA) and adds to the list yearly. Safe handling recommendations are then included in the package inserts for these drugs. The Oncology Nursing Society (ONS) and OSHA have also identified recommended practices in the area of hazardous drug administration. A study by Stover and Achutan (2011) evaluated one oncology/hematology unit's compliance with NIOSH and OSHA guidelines to protect against antineoplastic exposure and found that nursing staff did not always follow the recommendations of these organizations. For example, although double gloving and chemotherapy-resistant glove use is recommended by OSHA and NIOSH, 51 percent of nursing staff were not in compliance with this recommendation. About 10 percent reported they do not always wash their hands after handling these drugs. The study documented that several surfaces in patient's rooms, including bedside floors, bathroom surfaces, and IV poles, were contaminated with antineoplastic agents. Splashing or spilling may have caused these contaminations, with risks to nursing staff for direct dermal contact from surface contact, or indirect contact from inhaling or surface cross-contamination. Many staff members were unaware of these potential sources of contamination. The study also indicated that further education was needed for the nursing staff related to use of PPE in order to adhere to guidelines issued by OSHA and NIOSH (Stover & Achutan, 2011). In another study, NOISH (2015) examined predictors of adherence to safe handling practices for antineoplastic drugs in hospital nurses. This study analyzed survey responses from nurses employed by hospitals and found that training, familiarity with safe handling guidelines, and availability of engineering controls and personal protective equipment (PPE) were associated with better adherence to safe handling practices and fewer reported spills of antineoplastic drugs.
Nurses are frequently exposed to hazardous drugs (HD) in many nononcology settings but may not be aware of the risks and precautions when handling these drugs. Medications that have traditionally been used in oncology units, such as cytotoxic agents, are now used for other types of noncancerous conditions including autoimmune disorders because of their immunosuppressant effects. Hence, nurses are administering these drugs in general patient care units, clinics, and other settings. Chemotherapy and antitumor antibiotics that are cytotoxic may be infused directly into body cavities in the operating room during surgery, exposing operating room (OR) and postanesthesia personnel to these drugs. Methotrexate has been used as a treatment for ectopic pregnancy, which exposes obstetric nurses to this HD. Because methotrexate is usually administered by intramuscular (IM) injection for ectopic pregnancy, there is a risk of needle-stick injury and HD injection for the nurse administering the drug. Interferons are cytokines that are used in the treatment of multiple sclerosis. This class of drugs is listed as hazardous by NIOSH because of its effects on reproductive function. These medications are also typically administered by IM injection (Polovich & Gieseker, 2011). Concerns also arise over possible leakage of these drugs during intravenous (IV) administration as another source of occupational exposure.
Employers are required by OSHA to inform employees of the risks of any hazardous material in their workplace. Training is required related to these hazards, including HD administration, and safety data sheets (SDS), formerly known as material safety data sheets (MSDS), must be available to provide information about toxicities and measures to take in the event of a spill or accidental exposure. Protective environments must also be provided for employees along with policies and procedures for safe handling, including what PPE is required for HD administration. Polovich and Gieseker (2011) report that little is known about nononcology nurses' knowledge about safe handling precautions or whether they use safe handling recommendations, and that this should be a priority for future study. They advocate for “nurse safety” being just as important as patient safety. One way to accomplish this is to offer “alternate duty” for nurses who are pregnant, trying to conceive, or breastfeeding to ensure safety in this population of nurses who may be handling hazardous drugs as part of their regular duties.
Another area of concern regarding exposure to chemicals in the workplace has been recent evidence from a study that links miscarriages and other reproductive problems to nurses who have worked with antineoplastic drugs and sterilizing agents. Trossman (2012) reports that a study by a NIOSH researcher found that miscarriages were twice as likely in nurses exposed to these agents, as compared to those not exposed. X-ray exposure was also found to increase the miscarriage risk. ANA supports nurses' health and safety as a priority and backs the proposed federal Safe Chemicals Act that would reduce consumers' exposure to toxic chemicals and protect nurses and other workers from chemicals in the workplace.
Other workplace exposures of concern include cleaning products and lead and thimerosal (previously used as a preservative in multiple-dose vaccines) exposure for pediatric patients and pregnant healthcare workers. In one Massachusetts hospital, nurses and other employees experienced headaches and wheezing during floor stripping and waxing procedures. The Massachusetts Nurses Association, as the collective bargaining agent, worked to have high-efficiency particulate air (HEPA) filter fans used to absorb the fumes during this process after there was an unsatisfactory response from managers. Nurses are advised to document and inform managers of any symptoms related to hazardous workplace exposure (Watts, 2007). Such harmful exposures would also likely violate OSHA standards. In any case, employees are entitled to information contained in MSDS about any chemicals they are exposed to. NIOSH has listed occupational asthma as a high-priority concern.
In 2001, Brooks, a surgical technician in an OR, sued the manufacturer of a bone cement for failure to warn of product dangers that she was exposed to for several years (Carol Jean Brooks v. Howmedica, Inc., 2001). Brooks was exposed for about 4 days and 10 surgeries per week from 1982-1992 during the mixing process for Simplex P Radiopaque bone cement (Simplex). During the mixing process, a liquid and powder are mixed, releasing vapors classified as hazardous by OSHA. Brooks began experiencing a cough in 1990 and in 1991 was told she had asthma. An occupational health physician at the hospital reviewed the MSDS for the chemicals in the cement and talked with the manufacturer's chemist, but the investigation did not link her cough to Simplex. The employer did restrict her exposure to the chemicals in Simplex thereafter. However, Brooks was later diagnosed with occupational asthma caused by exposure to the chemical in the bone cement and was unable to work after 1995. Her employer, St. Luke's Hospital, intervened in the lawsuit seeking to recover compensation from defendant manufacturer Howmedica for workers' compensation benefits and other costs paid to Brooks.
Defendant Howmedica introduced evidence of stringent premarket approval for a new drug application (NDA) by the FDA, which approved its product labeling and package insert before the product was released to the market in 1971. This insert contained warnings of the highly volatile and flammable nature of the liquid, requiring adequate air circulation and to prevent excessive exposure to the vapors that may produce irritation to the respiratory tract, eyes, and possibly liver. Subsequently, they added more warnings for possible contact dermatitis and damage to soft contact lenses through exposure and recommended eliminating the maximum amount of vapor with adequate ventilation. Brooks testified that she had never read the product warnings in the package. The appeals court affirmed the judgment of the district court and granted summary judgment for the defendant manufacturer. The court found that federal laws regulating safety and labeling of medical devices and drugs (the 1976 Medical Devices Amendments to the Federal Food, Drug, and Cosmetic Act) preempted any state claim that would require different labeling and standards. Because this area is already regulated by the federal government, states cannot impose different regulations that may conflict with federal regulations. These different and conflicting state requirements could arise during lawsuits.
Even though Brooks was not able to successfully pursue a claim against the manufacturer, individual rights may arise under different theories of liability. Nurses are cautioned to be aware of workplace exposures to chemicals and to read all product labels and warnings. Nurse managers and supervisors should also be advocates of environmental health and safety to avoid any claims of corporate liability as a result of employee injury, and to ensure that OSHA and other standards are met.
Climate Change, Green, and Other Environmental Initiatives ⬆ ⬇
The Alliance of Nurses for Healthy Environments (ANHE) is a network of nurses around the country and world who act on the notion that the environment and health are inextricably connected. These nurses are from all practice settings and advocate for environmental health in workplaces and governmental institutions. Workgroups of the organization meet as a virtual community and center around education, practice, research, and policy/advocacy. They have created a website, EnviRN (http://envirn.org/), to network and share information as an active learning environment. A useful and comprehensive e-textbook is also available at the website to guide nurses in environmental awareness and practices. The ANHE has published “Environmental Health in Nursing” which is an open access e-textbook for nurses and other health professionals. Leading environmental health nursing experts have joined together to share their environmental health knowledge, expertise, and experiences in the publication. The electronic format provides direct links to authoritative resources such as the EPA, ToxNet, and WHO (Leffers et al., 2016).
The ANA has also been active in advocating for elimination or reduction of potentially harmful substances in the environment. For example, ANA provided testimony to an FDA panel of experts to support a ban on the use of Bisphenol-A (BPA), a chemical used to strengthen plastic in bottles, including baby bottles, and the lining of food cans. Concerns have been raised by government agencies about the effects of this chemical on neural functions and the behavior of fetuses, infants, and children (ANA, 2008).
Recent focus by the ANA has been on the role of nurses to promote a healthy world through recognition and action related to the effects of climate change. This includes the effects of heat and cold waves, global warming, rising sea levels, compromised air quality, natural disasters, crop failures and water restrictions among others. In the ANA's recently released position statement titled “Nurses' Role in Addressing Global Climate Change, Climate Justice, and Health” nurses are urged to recognize and address climate concerns in all areas of nursing practice (ANA, 2023). Many organizations join ANA in calling for urgent action related to climate change as a public health issue.
Nurses are called upon to integrate the science of climate and health into nursing education, research, and practice and to work with other health care professionals, community organizations, and policymakers to address the multiple health consequences of environmental degradation, extreme weather events, and other climate-related health impacts with evidence-based mitigation and adaptation actions, programs, and policies. (ANA, 2023, p.1)
Climate change affects the health and safety of patients, and contributes to disease and disability. Nursing programs are urged to include this content in nursing education curricula and to teach climate mitigation strategies, such as reducing carbon footprints and waste, and to provide eco-justice in the environment. Castner et al. (2024) suggest climate change activities and interventions as corporate social responsibility (CSR)-which aligns with nursing's commitment to equitable and planet-safe health-for individual nurses, nurse managers, and leaders to influence and contribute within their organizations. These authors make suggestions ranging from individual activities such as carpooling, to organizational activities such as reducing linen and other medical supply waste in the clinical environment, to professional organizations committing to climate change strategies. Inclusion of climate and health science and mitigation strategies in nursing curricula is also urged. Resources such as the federal Environmental Protection Agency (EPA), and the Agency for Healthcare Research and Quality (AHRQ) can be accessed for further information. The AHRQ recently published a primer on decarbonizing health care, which can support nurses' collective mitigation efforts (Castner et al., 2024).
The Agency for Toxic Substances and Disease Registry (ATSDR), a division of the CDC, began an initiative to support environmental health knowledge, skills, and awareness among nurses who serve individuals and communities. The vision of the initiative is to create a sustainable role for environmental health in professional nursing. The goal is to make environmental health an integral component of nursing practice, education, and research. Some accomplishments include development of educational tools and resources, such as online webcasts, environmental health curricula, and collaboration with other organizations for environmental health nursing roundtables.
Health Care Without Harm (HCWH) is another group working to improve environmental health and safety. Nurses play a key role in the organization's efforts, and there is an HCWH nurses' workgroup dedicated to implementing environmentally responsible practices in their hospitals. Initiatives include the elimination of mercury and the reduction or elimination of the use of toxic chemicals, such as polyvinyl chloride (PVC) and bis(2-ethylhexyl) phthalate (DEHP) contained in vinyl plastics used in medical devices such as feeding tubes. Consumer protection groups and professional organizations have also advocated for improved labeling of medical devices to warn of these dangers. In 2002, the FDA issued an advisory recommending the avoidance of using medical devices containing PVC and now warns healthcare providers to use non-PVC devices on patients who are at risk. Medical supply companies have responded by developing environmentally preferable medical products, such as latex- and PVC-free products. Recently, emphasis has been placed on designing hospitals and other patient care facilities with environmentally conscious materials and designs. Healthier and less toxic cleaning products and fragrance-free workplaces are also recommended.
References ⬆ ⬇
- American Nurses Association. (2008). ANA focus on BPA danger. American Nurse, 40(6), 15.
- American Nurses Association. (2015). Safe Patient Handling and Mobility Pamphlet. https://www.nursingworld.org/~498de8/globalassets/practiceandpolicy/work-environment/health--safety/ana-sphmcover__finalapproved.pdf
- American Nurses Association. (2021). Nursing scope and standards of practice (4th ed.). Silver Spring, MD: Author.
- American Nurses Association. (2023). ANA Position Statement: Nurses’ Role in Addressing Global Climate Change, Climate Justice, and Health, 1-18. Silver Spring, MD: Author. https://www.nursingworld.org/~4a64ad/globalassets/practiceandpolicy/nursing-excellence/ana-position-statements/social-causes-and-health-care/nursesroleinaddressingglobalclimatechangeclimatejusticeandhealth_bod-approved.pdf
- Carol Jean Brooks v. Howmedica, Inc., 273 F.3d 785; 2001 U.S. App. LEXIS 26357; CCH Prod. Liab. Rep. P16, 208 (2001).
- Castner , J., Schenk , E., & Cipriano , P. (2024). Climate change interventions. American Nurse Journal, 19(1), 10-17.
- Leffers , J, Smith , C., Huffling , K., McDermott-Levy , R., & Sattler , B. (Eds.). (2016). Environmental health in nursing. Alliance of Nurses for Healthy Environments, 1-166. www.enviRN.org
- The National Institutes for Occupational Safety and Health (NIOSH). (2015). Predictors of adherence to safe handling practices for antineoplastic drugs: A survey of hospital nurses. https://www.cdc.gov/niosh/updates/upd-12-09-15.html
- Noble , N., & Sweeney , N. (2018). Barriers to the use of assistive devices in patient handling. Workplace Health and Safety, 66(1), 41-48.
- Polovich , M., & Gieseker , K. E. (2011). Occupational hazardous drug exposure among non-oncology nurses. MEDSURG Nursing, 20(2), 79-97.
- Stover , D., & Achutan , C. (2011). Occupational exposures to antineoplastic drugs in an oncology-hematology department. Journal of Occupational and Environmental Hygiene, 8(1), D1-D6.
- Tillotson v. St. Joseph Medical Center, 347 S.W. 3d 511(2011).
- Trossman , S. (2012). Hazardous conditions: Study links miscarriages and working with certain drugs. American Nurse, 44(2), 1, 7.
- Tucker , L., & Parker , K. (2022). 10-year weight gain in 13,802 US adults: The role of age, sex, and race. Journal of Obesity, 1-10. doi: 10.1155/2022/7652408
- Watts , N. (2007). Newton Wellesley RNs address hazards of environmental cleaning chemicals. Massachusetts Nurse, 78(4), 10.
Additional Resources ⬆