Retinoblastoma: A malignant tumor of the retina that appears as a white, nodular mass that breaks through the internal limiting membrane into the vitreous (endophytic), as a subretinal mass lesion often underlying a serous retinal detachment (exophytic), or as a diffusely spreading lesion simulating uveitis (diffuse infiltrating). Iris neovascularization is common with large tumors. Aqueous and vitreous seeding may occur. Cataract is uncommon, and the eye is normal in size. May be bilateral, unilateral, or multifocal. Diagnosis is usually made in patients under 5 years of age, with a mean age of 18 months. A family history may be elicited in about 10%.
Toxocariasis: A nematode infection that may appear as a localized, white, elevated granuloma in the retina or as a diffuse endophthalmitis. Associated with localized inflammation of ocular structures, vitreous traction bands and related macular dragging, traction retinal detachment, and cataract. It is rarely bilateral and is usually diagnosed between 6 months and 10 years of age but may present in adults as well. Paracentesis of the anterior chamber may reveal eosinophils; serum enzyme-linked immunosorbent assay (ELISA) test for Toxocara organisms is positive. The patient may have a history of contact with puppies or of eating dirt. Toxocariasis may also be acquired prenatally and present as a congenital infection.
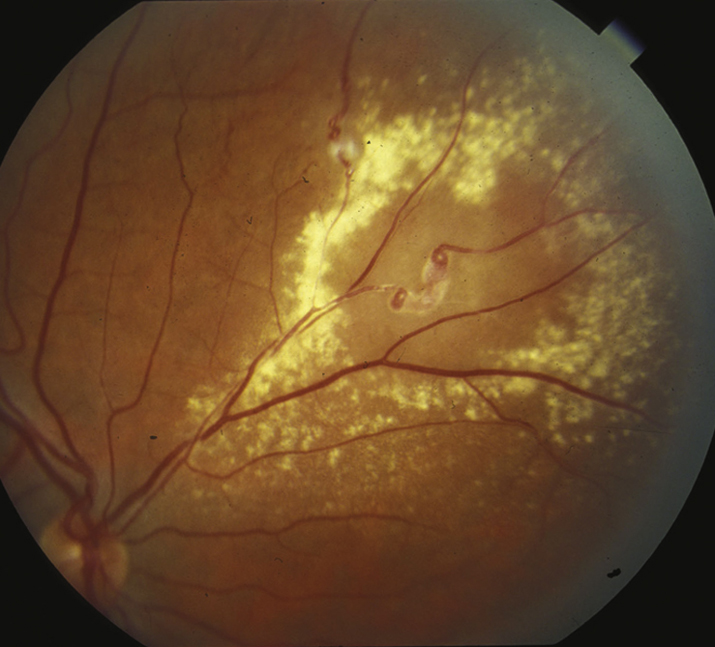
Coats disease (see Figure 8.1.2): A retinal vascular abnormality resulting in microaneurysms and macroaneurysms of the retinal vessels, usually in the inferotemporal periphery. Xanthocoria may develop secondary to an exudative, often bullous retinal detachment associated with yellow-colored, lipid-rich subretinal fluid or to extensive, yellow intraretinal and subretinal exudate. Usually develops in boys during the first decade of life; more severe cases occur in early childhood. Coats disease is rarely bilateral. No family history.
Persistent fetal vasculature (PFV) (previously known as persistent hyperplastic primary vitreous): A developmental ocular abnormality with failure of regression of the fetal hyaloid complex, often with a fibrovascular stalk from the optic nerve to lens and anterior segment. May only present with anterior or posterior findings. It is usually associated with a small eye. Typically there is a membrane behind the lens that places inward traction on elongated ciliary processes. A cataract is noted at birth or early in life. The membrane and lens may rotate anteriorly, shallowing the anterior chamber and resulting in secondary glaucoma. Traction retinal detachment can occur. Usually unilateral. No family history or other risk factors.
Pediatric cataract: Opacity of the lens present at birth or in first months of life; may be unilateral or bilateral. There may be a family history or an associated systemic disorder. See 8.8, PEDIATRIC CATARACT.
Retinal astrocytoma: A sessile to slightly elevated, yellow-white retinal mass that may be calcified and is often associated with tuberous sclerosis complex and rarely neurofibromatosis. May occur on the optic nerve head (giant drusen) in patients with tuberous sclerosis.
Retinopathy of prematurity (ROP): Predominantly occurs in premature children. Leukocoria is usually the result of a retinal detachment. See 8.2, RETINOPATHY OF PREMATURITY.
History: Age at onset? Family history of one of the conditions mentioned? Prematurity? Contact with puppies or history of eating dirt?
Complete ocular examination, including a measurement of corneal diameters (look for a small eye), an examination of the iris (look for neovascularization), and an inspection of the lens (look for a cataract). A dilated fundus examination and an anterior vitreous examination are essential.
Any or all of the following may be helpful in diagnosis and planning treatment:
B-scan ultrasonography (US), especially if there is no view of the fundus. This can be used to look for calcification within a suspected tumor, a persistent stalk from the optic disc to the back of the lens, or a retinal detachment.
Intravenous fluorescein angiogram (useful for evaluation of Coats disease, ROP, retinoblastoma).
Magnetic resonance imaging (MRI) (or computed tomography [CT]) of the orbit and brain, particularly for bilateral cases of retinoblastoma or those with a family history. Also advised in cases of advanced Coats disease. MRI is preferable for retinoblastoma to reduce radiation exposure, given risk of future malignancy.
Serum ELISA test for Toxocara (positive at 1:8 in the vast majority of infected patients).
Systemic evaluation by pediatrician, especially if concern for retinal astrocytic hamartoma, retinoblastoma, or cataract secondary to systemic disease.
Anterior chamber paracentesis and serum ELISA test for evaluation of toxocariasis (serum antibody test positive at 1:8 in the vast majority of patients infected with Toxocara). See Appendix 13, ANTERIOR CHAMBER PARACENTESIS.
May need examination under anesthesia (EUA) in young or uncooperative children, particularly when retinoblastoma is being considered as a diagnosis. If there is concern for inherited retinoblastoma, screening examination can be performed in the office within 1 to 2 weeks of birth. See 8.8, PEDIATRIC CATARACT, for a more specific cataract workup.
NOTE:
Anterior chamber paracentesis in a patient with a retinoblastoma should be avoided as it could lead to tumor cell dissemination.
Treatment⬆⬇
Retinoblastoma: Chemoreduction, intra-arterial chemotherapy, intravitreal chemotherapy, cryotherapy, thermotherapy, laser photocoagulation, or plaque radiotherapy. These treatment modalities are typically used in combination. Enucleation is reserved for cases not amenable to the above treatment options or in advanced unilateral cases. Systemic chemotherapy is used in metastatic disease. External irradiation is rarely used as it is associated with a high incidence of secondary tumors later in life.
Toxocariasis:
Steroids (topical, periocular, or systemic routes may be used, depending on the severity of the inflammation).
Consider vitrectomy when vitreoretinal traction bands form or when the condition does not improve or worsens with medical therapy.
Consider laser photocoagulation of the nematode if it is visible.
Antihelminth therapy (albendazole) only warranted for systemic disease.
Coats disease: Fluorescein angiography–guided laser photocoagulation to leaking vessels and aneurysms and can consider intravitreal anti-VEGF agents in addition to the laser if there is posterior involvement. External drainage of the subretinal fluid may be beneficial for severe retinal detachment.
PFV:
Cataract removal and retrolental stalk resection, with posterior vitrectomy depending on extent of posterior involvement.
Treat any amblyopia, although visual outcome is often poor secondary to numerous factors such as foveal hypoplasia, anisometropia, optic nerve hypoplasia, and sensory deprivation.
Variable, depending on the diagnosis. If any concern for heritable disorders, consider referral to ophthalmic genetics and screening of family members.
 NOTE:
NOTE: