- Reduce dietary protein consumption and substitute artificially flavored solutions of essential amino acids without arginine (e.g., arginine-restricted diet). Monitor serum ammonia levels.
- Supplemental vitamin B6 (pyridoxine). The dose is not currently established; consider 20 mg/d p.o. initially and increase up to 500 mg/d p.o. if there is no response. Follow serum ornithine levels to determine the amount of supplemental vitamin B6 and the degree to which dietary protein needs to be restricted. Serum ornithine levels between 0.15 and 0.2 mmol/L are optimal.
 NOTE: NOTE: |
Only a small percentage of patients are vitamin B6 responders. |
- Choroideremia: Males present in the first to second decade of life with nyctalopia, followed by insidious loss of peripheral vision. Decreased central vision occurs late. In males, early findings include dispersed pigment granules in the periphery with focal areas of RPE atrophy. Late findings include total absence of RPE and choriocapillaris. No bone spicules. Retinal arteriolar narrowing and optic atrophy can occur late in the process. Constriction of visual fields, normal color vision, markedly reduced ERG. Female carriers have small, scattered, square intraretinal pigment granules overlying choroidal atrophy, most marked in the midperiphery. No effective treatment for this condition is currently available. Darkly tinted sunglasses may ameliorate symptoms. X-linked recessive. Consider genetic counseling.
- Vitamin A deficiency: Marked night blindness. Numerous small, yellow-white, well-demarcated spots deep in the retina seen peripherally. Dry eye and/or Bitôt spots (white keratinized lesions) on the conjunctiva. See 13.7, VITAMIN A DEFICIENCY.
- Zinc deficiency: May cause abnormal dark adaptation (zinc is needed for vitamin A metabolism).
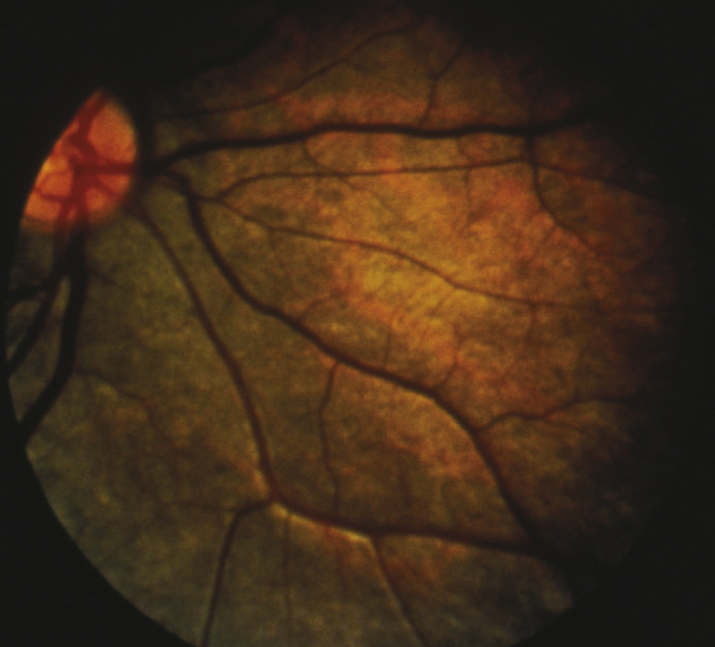
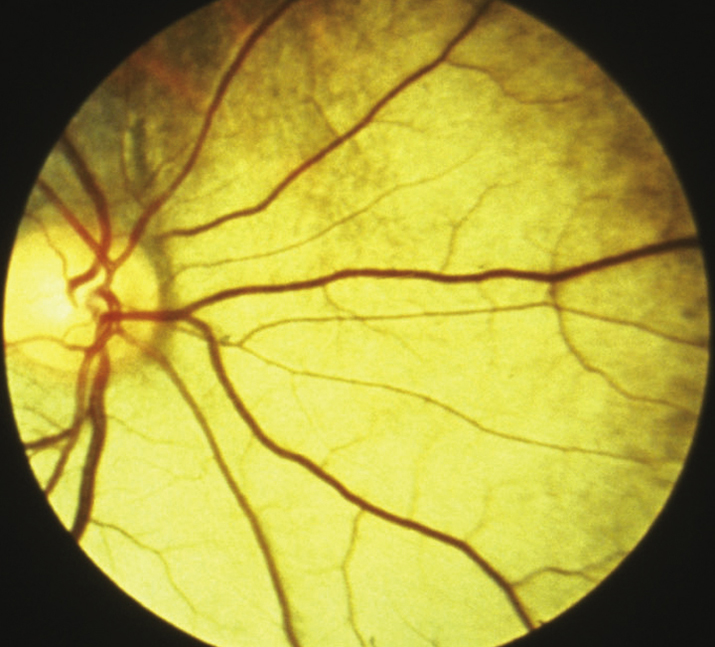
- Congenital stationary night blindness: Night blindness from birth, normal visual fields; may have a normal or abnormal fundus, not progressive. Paradoxic pupillary response. One variant is Oguchi disease, characterized by the Mizuo phenomenon—the fundus has a tapetum appearance in the light-adapted state but appears normally colored when dark-adapted (may take up to 12 hours) (see Figures 11.28.3 and 11.28.4).
- Undercorrected myopia: The most common cause of poor night vision.
- Gyrate atrophy: Nyctalopia and decreased peripheral vision usually presenting in the first decade of life, followed by progressive constriction of visual field. Scalloped RPE and choriocapillaris atrophy in the midperiphery during childhood that coalesces to involve the entire fundus, posterior subcapsular cataract, high myopia with astigmatism. Constriction of visual fields and abnormal to nonrecordable ERG. Plasma ornithine level is 10 to 20 times normal; lysine is decreased. Consider ERG and IVFA if the ornithine level is not markedly increased. Autosomal recessive.