Critical
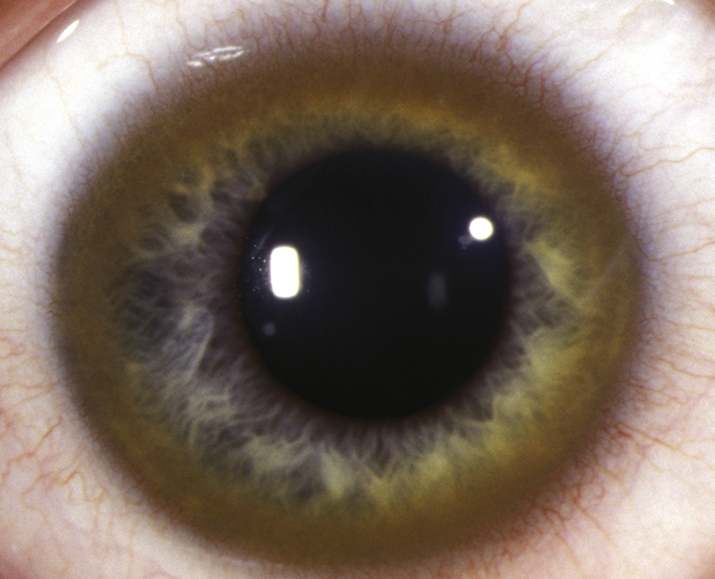
Kayser–Fleischer ring: 1- to 3-mm, brown, yellow, green, or reddish band that represents copper deposition in the peripheral Descemet membrane (see Figure 13.10.1). Present in 50% to 60% of patients with isolated hepatic involvement and more than 90% of patients with neurologic manifestations. First appears superiorly (may only be visible on gonioscopy) and eventually forms a ring involving the entire corneal periphery extending to the limbus. Anterior-segment optical coherence tomography (OCT) may be useful in detecting early Kayser–Fleischer rings that are not readily detected on slit lamp examination; appears as linear hyperreflective material on Descemet membrane.
Other
“Sunflower” cataract: Ring or stellate yellow, brown, or reddish anterior capsule opacity due to copper deposition under the lens capsule.