Mild-to-moderate foreign body sensation, photophobia, and tearing. No history of red eye. Usually bilateral with a chronic course of exacerbations and remissions, but may not be active in both eyes at the same time.
Critical
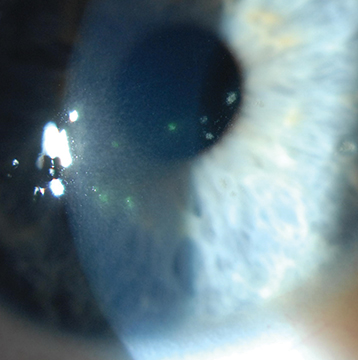
Coarse stellate gray-white corneal epithelial opacities that are often central, slightly elevated, and stain lightly with fluorescein. Underlying subepithelial infiltrates may be present (see Figure 4.8.1).
Figure 4.8.1: Thygeson superficial punctate keratitis.
Other
Minimal-to-no conjunctival injection, corneal edema, anterior chamber reaction, or eyelid abnormalities.
See 4.1, Superficial Punctate Keratopathy.
Weekly during an exacerbation and then every 3 to 6 months. Patients receiving topical steroids require intraocular pressure (IOP) checks every 4 to 12 weeks.