Description
- Circulating blood is necessary for meeting the nutritional demands of tissues, removing wastes, delivering hormones, and keeping an environment in all tissue that is optimal for cell function and survival.
- The rate of blood flow to tissue is dependent on its nutritional needs. Cardiac output (CO) is maintained by alterations in the heart and blood vessels.
- CO is the amount of blood pumped out of the heart into the aorta each minute; it is blood flow.
- Average CO for adults: 5.6 L/minute for males, 4.9 L/minute for females.
- Varies with age, physical activity, body surface area (BSA), and metabolism.
- Cardiac index (CI). Because CO increases proportionally with BSA, CI can be used as a measurement. Average CI is approximately 3 L/min/m2.
- Extrinsic factors that control CO:
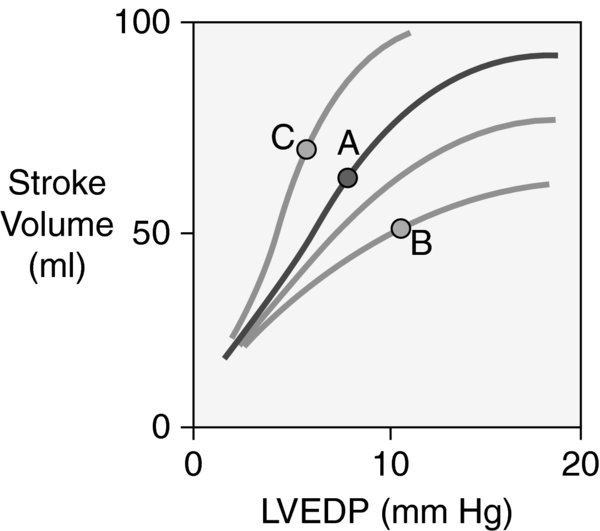
The Frank–Starling law is the heart's built-in mechanism to control CO. It states that increased venous return (end diastolic volume; EDV) increases wall stretch of the heart chambers and myocardial cells; this allows cardiac muscle to have greater contractile force resulting in an increase in SV and therefore CO (Figure 1). An analogy is a bow and arrow; the greater the stretch, the greater the force exerted on the arrow. However, past a certain EDV, further filling can become ineffective (will exceed troponin and myosin overlap and result in a decrease in contractile force and decrease in CO).
FIGURE 1. Effects of changes in afterload on Frank-Starling curves.
A shift from A to B occurs with increased afterload, and from A to C with decreased afterload.
From Richard Klabunde. www.cyphysiology.com, 2011, with permission.- Stretch of the sinus node in the wall of the right atrium (RA) has a direct effect on heart rate (HR), increasing HR by as much as 10–15%.
- The Bainbridge reflex is a nervous system reflex, also initiated by a stretched RA, that increases HR.
- In translation, the heart, itself, is not principally responsible for CO. Under normal, unstressful situations, CO is controlled by extrinsic factors, mainly venous return.
- Intrinsic factors that control CO:
- HR depends on the diastolic interval. The diastolic interval is controlled by the sinoatrial (SA) node pacemaker (dependent on calcium and potassium channels).
- EDV depends on filling pressure, filling time, and ventricular compliance.
- Longer filling times
 increases EDV.
increases EDV. - Increased ventricular compliance increased EDV.
- Longer filling times
- End systolic volume (ESV) depends on
- HR: Increased HR is secondary to increased calcium in pacemaker/myocardial cells; this also results in increased contractility, and decreased ESV.
- Contractility: Increased inotropy will result from increases in calcium within myocardial cells, with resultant increases in contractility and HR and decreases in ESV.
- Preload: Increased EDV increases stretch and consequently contractile forces, with a resultant decrease in ESV.
- Afterload: Increases prevent the heart from emptying with resultant increases in ESV.
- Ejection fraction (EF) is a term that is utilized to describe the systolic function of the heart in terms of SV and EDV. It is the percentage of blood that is ejected by the ventricles with heart beat; normal is 55–65%.
- Arteries: High pressure, high flow, strong vascular walls. Function: Transport of blood to tissues.
- Arterioles: Small branches of arteries, variable flow and pressure. Function: Control conduits; muscular walls are able to contract and dilate to vary local blood flow in tissue beds.
- Capillaries: Small thin-walled vessels. Function: Nutrient/waste exchange site.
- Venules: Collect blood from capillaries and form progressively larger veins.
- Veins: Low volume, thin walls, low pressure. Function: Return blood back to the heart, serves as a reservoir of blood, can also contract/dilate depending on circulatory needs.
- SA node: Located at the junction of the SVC and RA. Serves as the cardiac pacemaker, largely dependent on calcium channels.
- Cardiac myocytes: Striated muscle with gap junctions that allow muscle fibers to function as a unit.
- Distribution of CO to organs: Brain 15%, heart 5%, kidneys 20%, liver 25%, muscle 15% (can increase to up to 65% with exercise), skin 10%, bones/fat/other 15%.
Physiology/Pathophysiology
- High CO states (usually as a result of decreased SVR or shunts): Activates the renin-angiotensin system and increases sympathetic output with resultant increases in heart rate, vasoconstriction, and salt and water retention. Leads to ventricular remodeling and failure.
- Beri beri: Thiamine deficiency that leads to peripheral vasodilation, increased CO, salt retention, and edema. Because of a high CO, the myocardium sustains overuse injuries that can lead to tachycardia, edema, high pressures, and chest pain.
- AV shunt (fistula): Reduces SVR and arterial BP; this is compensated by increasing the CO.
- Hyperthyroid: Increased metabolism results in decreased SVR that is compensated by increasing the CO.
- Anemia: Decreases blood viscosity and SVR along with vasodilation from increased nitric oxide synthase.
- Obesity: Increases blood volume and CO to sustain excess body mass.
- Cirrhosis: Results in splanchnic vasodilation, and also development of shunts.
- Pregnancy: Increased metabolic demand is compensated for with an increase in the circulating blood volume and HR.
- Shock: The release of cytokines results in extreme vasodilation and decreased SVR; this is compensated for by an increase in CO.
- Low CO states:
- Hypovolemia: Decreased venous return and EDV result in decreased CO
- Acute venous dilatation: similar to hypovolemia, with decreased EDV.
- Obstruction of large veins: Again, decreased venous return leading to a decrease in the EDV
- Arrhythmias: Decreased ventricular filling time and decreased SV lead to decreased CO.
- Decreased metabolic rate
- Late sepsis: Inadequate tissue oxygenation leads to multiorgan failure, including heart failure.
- Regional wall motion abnormalities due to ischemia: Decreased contractility resulting in decreased EF.
- Valvular disease: Leads to structural changes in the heart muscle and eventual decreases in systolic function (EF).
- Cardiomyopathy: Impaired ventricular compliance resulting in decreased contractility via Frank–Starling law.
- Mean arterial pressure (MAP) is the perfusion pressure to organs. MAP = CO × SVR.
- As preoperative clinicians, we need to understand the interrelationship of these physiologic parameters in order to intervene appropriately, as too high or too low CO can be detrimental to the patient.
- Measuring CO. In the perioperative setting, this is typically done via invasive monitoring. Furthermore, CO measurements do not provide information about end-organ blood flow and oxygen utilization by tissue. Currently, the only monitor that addresses this is mixed venous oxygen saturation (SvO2).
- Thermodilution technique via the Swan–Ganz catheter is frequently used.
- Echocardiography measures changes in the ventricular volumes to calculate stroke volume, which is then multiplied by the HR.
- Velocity encoded MRI. Very accurate method to measure velocity based on detection of changes in the phase of proton precession.
- Arterial line waveform analysis. Area under the curve equals work or stroke volume.
- Invasive pulse pressure, involves inserting a manometer in the artery, the waveform is analyzed and CO calculated.
- SvO2: Blood samples are collected viaa pulmonary artery catheter. Reflects balance of oxygen delivery, determined by CO, and oxygen consumption.
- Receptors
 1: Directly increases HR (chronotropy) by stimulating the SA node, and increases contractility (inotropy) and automaticity of cardiac muscle all increase CO.
1: Directly increases HR (chronotropy) by stimulating the SA node, and increases contractility (inotropy) and automaticity of cardiac muscle all increase CO.- 2: Dilates arteries to skeletal muscle which
 afterload and
afterload and  stroke volume and therefore CO, but to a lesser degree than 1 receptors.
stroke volume and therefore CO, but to a lesser degree than 1 receptors.  1: Principle effect is vasoconstriction which increases the SVR.
1: Principle effect is vasoconstriction which increases the SVR.- Dopamine: Increases HR and BP. Low doses: Vasodilates and increases renal blood flow. Intermediate doses: Increases CO by positive chronotropy and inotropy. High doses: Acts as a pressor causing vasoconstriction.
- Drugs and receptors
- Epinephrine: Has both and activity
- Norepinephrine: Predominantly activity
- Dobutamine: 1 selective
- Isoproterenol: 1 and 2
- Phosphodiesterase inhibitors: Increases contractility, pulmonary, and systemic vasodilation
- Calcium: Directly increases myocardial contractility
- Glucagon: Acts as a positive inotrope and increases CO. Also, decreases SVR by arterial and venous vasodilation
- Epinephrine: Has both
- Hypotension. Workup should include an assessment of preload, afterload, contractility, HR, and rhythm in light of the clinical picture. The ASA/SCA recommends obtaining transesophageal echocardiography when the diagnostic information will alter the management – this includes unexplained persistent hypotension.
- Decreased CO likely results in a longer IV drug circulation time and slower onset of action. Conversely, volatile agents have a quickened onset due to a more quickly increased alveolar concentration (less volatile agent is carried away). Increased CO results in a faster IV drug onset time, while volatile agents have a slower onset (slower increase in alveolar concentrations).
- OHM's law: V = I/R or Flow = Pressure/Resistance
- CO = MAP/SVR (PVR for right heart, SVR for left heart)
- CO = SV × HR
- SV = EDV – ESV
- Fick principle: CO = VO2/(CaO2 -CvO2); where VO2 is oxygen consumption, CaO2 is arterial oxygen concentration, and CvO2 is venous oxygen concentration
- CI = CO/BSA
- BSA = 0.20247 × height (m)0.725 × weight (kg)0.425