- An arterial line is an invasive monitor that provides:
- Beat-to-beat numeric blood pressure values
- A waveform with arterial pressures (y-axis) as a function of time (x-axis)
- A means to attain arterial blood gas sampling
- An electromechanical transducer is coupled to the patient via a fluid column that is generally composed of normal saline heparin (4 units/mL).
- During the cardiac cycle, blood ejected from the left ventricle (LV) flows into the vascular tree. A pressure wave is transmitted through the vessels temporally leads the flow of blood.
- Measurement of pressure occurs at the level of the transducer, not the location of the cannula. This is in contrast to noninvasive blood pressure (NIBP) measurements, where measurement occurs at the level of the cuff.
- The arterial waveform is a measure of pressure does not necessarily correlate to cardiac output (flow). for example, in patients with poor cardiac output a high systemic vascular resistance (SVR), pressure will be normal but perfusion inadequate.
- Anacrotic limb describes the first phase of the arterial pulse cycle represents ventricular ejection of blood. The highest point corresponds to the systolic blood pressure.
- Dicrotic limb describes the downstroke of the waveform; it begins at the peak, continues through the dicrotic notch, ends at the diastolic baseline. The dicrotic notch coincides with closure of the aortic valve the end of LV ejection. It is a result of the reflection of the pressure wave created when the forward flow of blood out of the LV stops the elastic recoil of the aorta forces blood back against the closed aortic valve. Pressure decay is the drop in pressure over time (dP/dT) from the dicrotic notch to diastolic pressure; it is a function of SVR.
- Steep slopes correspond to decreased SVR/afterload. The waveform appears narrow.
- Dampened slopes correspond to increased SVR/afterload. The waveform may appear widened.
- The highest fidelity of readings waveform data occurs when utilizing:
- The largest diameter catheter that does not obstruct the lumen of the vessel
- The shortest length of high pressure (stiff walled) tubing between the transducer the patient
- Tubing that is free of gas bubbles
- Tubing that is free of other obstructions such as clotted blood
- A catheter that is placed closer to the central vascular tree
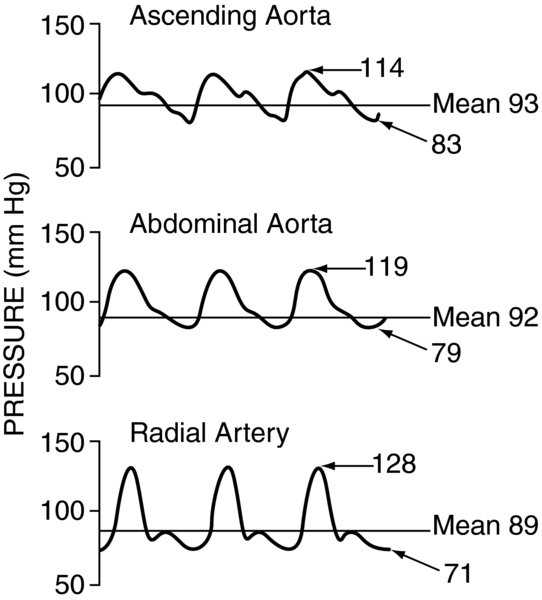
Reflection deflection occur as blood flows through the vasculature. Because the arterial system undergoes constant pressure adjustments as well as has several bends branches, the flow of blood is turbulent as well as laminar. Turbulent flow results in pressure waves being reflected much like waves in a pool of water are reflected off the concrete side. This results in increased systolic pressures decreased diastolic pressures in the more distal arteries; the mean pressure is only minimally affected. Alternatively, if the vessels were straight, had no branches, flow would be laminar the pressures would not change in the more distal arteries.
FIGURE 2. Arterial line tracing from proximal to distal sites.
Systolic pressures increase, diastolic pressures decrease, while mean pressures remain mostly unchanged.

- Although any artery can be used, the risk of distal thrombosis limits catheter placement to larger vessels with adequate collateralization.
- The radial artery is the most common location for arterial monitoring.
- The ulnar artery is more difficult to cannulate because it is deeper at the wrist. It should not be used if the ipsilateral radial artery has been punctured.
- Some suggest the use of the Allen Test to assess the adequacy of collateralization of the h.
- Recent studies have called this into question if there is doubt, vascular ultrasound should be used (1).
- Use of the femoral artery must be balanced against concerns of site line infection, pseudo-aneurysm formation, or distal embolization from plaque rupture.
- Other less frequently used sites for arterial wave monitoring include axillary, brachial, dorsalis pedis vessels.
- In neonates temporal umbilical arteries are used.
- Dicrotic notch: The notch is a result of the reflection of the pressure wave created when the forward flow of blood out of the LV stops the elastic recoil of the aorta forces blood back against the closed aortic valve.
- Patients with severe aortic insufficiency will have an indistinct notch. Since the aortic valve is incompetent, blood flows freely backward, no such pressure wave is generated.
- A flat or absent notch may suggest low intravascular volume.
- A low or late notch may correlate to decreased SVR.
- Heparin-induced thrombocytopenia (HIT): In some patients, chronic exposure to heparin can result in HIT (2). HIT results in thrombosis, not bleeding. Sodium citrate has been used as a substitute for heparin in the flush (3).
- Thrombosis is an unusual complication but potentially devastating if it results in prolonged ischemia (4). First-line therapy is systemic anticoagulation. Some studies have been performed showing thrombolytics are effective as second-line therapy (5).
- Temporary occlusion of the radial artery following arterial line placement is not infrequent is reported in 1.5–35% (mean 19.7%) of studies on the subject. Generally temporary occlusion has no serious consequences (6).
- Placement of arterial waveform monitoring is common when continuous beat-to-beat blood pressure measurement is indicated. Changes in the waveform can be useful in cases where rapid changes in volume status are occurring.
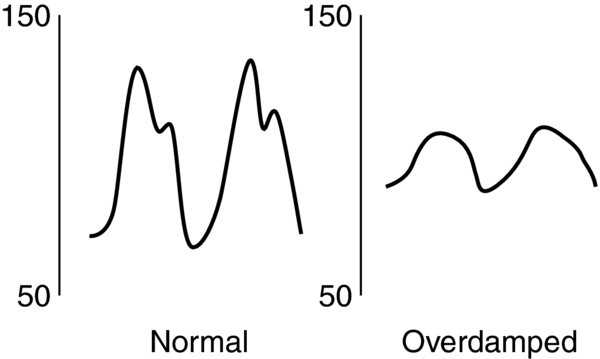
- Dampened waveforms result in underestimation of the blood pressure can be seen with:
- Lumen occlusion due to thrombosis, clots, air bubbles, or kinking
- Loss of backpressure from the flush solution (low flush bag pressure, no fluid in pressure bag)
- Troubleshooting involves inspection of the system starting from the placement site (if possible) back to the electronics. On opening the transducer to air, the reading should drop to zero. If not, this indicates the possibility of baseline drift the system should be re-zeroed. Next, the system should be flushed. If the reading does not move over 300 mmHg, then the pressure bag should be checked. Otherwise the system should be inspected distal to the transducer for obstructions, disconnections, or leaks.
Tubing: overly compliant, distensible; incorrect tubing
FIGURE 3. Dampened tracing results in decreased systolic pressures, increased diastolic pressures, while mean pressures remain mostly unchanged.
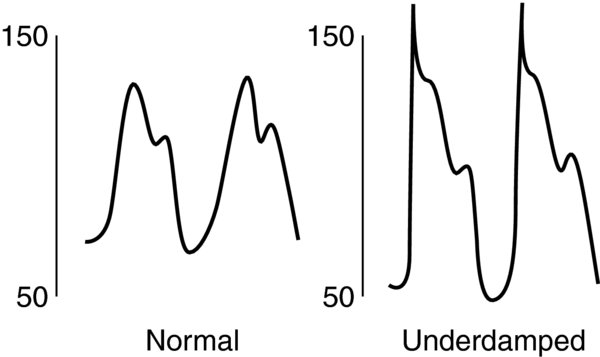
- Under-dampened or resonant waveforms result in overestimation of the blood pressure can occur due to:
- Tubing: Long, noncompliant, overly-stiff.
- “Ringing” describes exaggerated highs lows that can occur when the measurement system comes close to the natural underlying harmonic frequency of the waveform.
Increased SVR
FIGURE 4. Under-dampened or resonant tracing results in increased systolic pressures, decreased diastolic pressures, while mean pressures remain mostly unchanged.
- The electromechanical system must be zeroed prior to use by opening the transducer to air. for neurosurgical cases, or cases where the patient is in the sitting position, the zero reference is commonly set to the Circle of Willis at the level of the ear. Otherwise, the zero reference is placed at the level of the heart. If the transducer is not physically attached to the OR bed, the level must be adjusted when changes in patient position or vertical height are made.
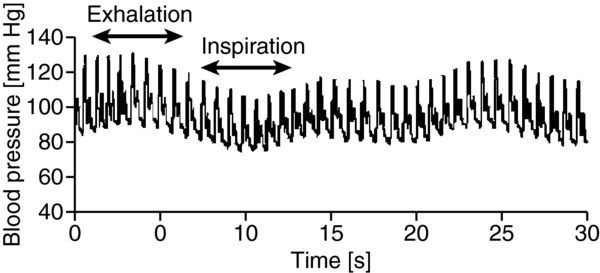
- Stroke volume variation describes changes in the systolic diastolic pressure that correlate with the respiratory cycle.
- Mechanical ventilation: Positive pressure inspiration corresponds with an increase in airway pressures, compression of intrathoracic veins, a decrease in transmural blood flow. As a result, with inspiration, there is decreased preload that corresponds to decreased blood pressure. Conversely, exhalation corresponds to a decrease in airway pressures with increases in blood pressure.
Spontaneous ventilation: Exhalation the end of inspiration correspond to an increase in airway pressures, compression of intrathoracic veins, a decrease in transmural blood flow.
FIGURE 5. Stroke volume variation with mechanical ventilation.
Exhalation corresponds to decreased intrathoracic pressures, allowing blood to return to the heart (increased preload, with resultant increase in cardiac output blood pressure). Inspiration corresponds to increased intrathoracic pressures with resultant decreases in blood return to the heart (decreased preload that causes decreases in stroke volume, cardiac output, blood pressure).
- Arterial line placement can be aided by ultrasound, but this is usually reserved for femoral cannulation of pediatric patients select adults.
- Newer methods of cardiac output monitoring use a peripheral arterial line the pressure waveform to calculate cardiac output. Unlike thermodilution methods, these devices use advanced algorithms to assess vascular tone sensing technology to indirectly measure SVR.
- Arterial transducers are built to continually infuse a small volume (3 mL/hr) of flush solution to reduce cannula thrombosis.