Description
- Subclavian steal syndrome is a phenomenon of transient cerebral ischemic attacks following ipsilateral arm exercise in the presence of severe stenosis (>80%) or occlusion of the subclavian artery proximal to the origin of the vertebral artery.
- During exercise, blood flows retrograde from the ipsilateral vertebral artery to the distal subclavian artery to supply the arm; in doing so, blood is diverted from the circle of Willis can result in transient cerebral ischemia.
- Coronary–subclavian steal syndrome is a rare complication following use of the left internal mammary artery (LIMA) graft for coronary artery bypass (CABG) in the presence of severe proximal stenosis in the left subclavian artery. This may produce reversal of blood flow from the heart to the ipsilateral arm during exercise that leads to angina pectoris.
- Subclavian steal is a flow-related phenomenon.
- At rest, when a proximal occlusion develops in the subclavian artery, the arm becomes dependent on the collateral vessels from the head, shoulder, neck, particularly retrograde flow from the ipsilateral vertebral artery.
- When the arm is exercised, the blood vessels dilate create a low resistance vascular bed. More blood flows from the contralateral vertebral artery to the basilar artery there is increased retrograde flow into the ipsilateral vertebral artery down to the subclavian artery to supply the arm.
- Coronary–subclavian steal can happen when patients have a coronary bypass using an in situ LIMA graft, in conjunction with significant stenosis in the proximal left subclavian. Thus, retrograde flow can occur direct the blood away from the heart to the arm.
- Normally, BPs are similar in both arms. A significant discrepancy raises a possibility of stenosis in a subclavian artery, or coarctation of the aorta.
- The vertebral arteries arise from the superior aspect of the proximal subclavian artery feed into the basilar artery, which is part of the circle of Willis.
- The cerebral collateral conduits are mainly formed by the circle of Willis. It is an arterial ring surrounding the optic chiasma hypothalamus.
- Anteriorly, it is formed by the left right anterior cerebral arteries that arise from the left right internal carotid arteries; they are “linked” by the anterior communicating arteries.
- Posteriorly, it is formed by the division of the basilar artery into the left right posterior cerebral arteries.
- Laterally, the left right posterior communicating arteries join the left right posterior cerebral arteries to the internal carotid arteries.
- The internal mammary artery arises from the inferior aspect of the proximal subclavian artery, opposite the vertebral artery.
Physiology/Pathophysiology
- The most common cause of proximal occlusive lesions in the subclavian arteries is atherosclerosis. The most common sites are the
- Left subclavian artery (62%)
- Right subclavian artery (28%)
- Right innominate artery (10%)
- Other less common causes include
- Takayasu disease
- Temporal arteritis
- Status post surgical repair of coarctation of the aorta
- Congenital lesions of the aortic arch or subclavian artery
- Status post Blalock–Taussig procedure for tetralogy of Fallot
- Compression of the subclavian artery in the thoracic outlet
- Not all retrograde flow through the vertebral artery leads to neurologic symptoms; the majority of time it is asymptomatic. It usually only becomes symptomatic when occlusive lesions in the cerebral collateral conduits are present. 80% of patients with subclavian steal syndrome have contralateral vertebral or carotid disease.
- Neurological symptoms in subclavian steal syndrome usually resolve after discontinuing exercise of the arm. Common symptoms include
- Vertigo (50%)
- Diplopia (19%)
- Syncope (18%)
- Dysarthria (12.5%)
- Ataxia
- Blurring of vision
- Perioral numbness
- Paresthesia
- Infarction is rare
- Other symptoms:
- Exercise-induced arm pain
- Absent or diminished pulse in the ipsilateral arm a significantly unequal systolic BP from one side to the other (>20 mm Hg).
- Bruit in the supraclavicular fossa
- A recurrence of angina in a patient who has had a coronary bypass using a LIMA graft with presence of stenosis in the proximal left subclavian artery indicates a possibility of coronary–subclavian steal.
- The most common etiology is atherosclerosis. Thus, subclavian stenosis is associated with an increased total mortality cardiovascular disease mortality after adjusting for common risk factors (2). They share the same risk factors as those with coronary artery disease:
- Advanced age
- Male sex
- Family history
- Cigarette smoking
- Hypercholesterolemia
- Diabetes mellitus
- Hypertension
- Hyperhomocysteinemia
- Less common etiologies need to be identified if present. They may dictate special anesthetic planning special requirements on intraoperative monitoring.
- Diagnostic studies are done not only to confirm the diagnosis but also to ensure patent proximal common carotid distal subclavian arteries to rule out any coexisting lesions in the collateral pathways.
- Duplex ultrasonography (combined two-dimensional ultrasound pulse-wave Doppler) of the neck arteries. A coexisting severe carotid stenosis generally requires that a carotid endarterectomy be performed first then a reevaluation of any persistent neurologic symptoms be made.
- Four-vessel cerebral angiography
- CT angiography
- Magnetic resonance angiography in patients with renal insufficiency
- Conservative treatment includes controlling hypertension, lipid modification, glycemic control in diabetes, smoking cessation, antiplatelet treatment with aspirin.
- Surgical treatment is only indicated for symptomatic patients.
- Endovascular angioplasty /or stenting of the subclavian artery has a success rate of 86–93%. The complication rate is about 3–17%. The restenosis rate is about 0–16% in stenting after 12–48 months. Stenting requires postoperative aspirin clopidogrel for 6–12 months to reduce the risk of restenosis.
- Extrathoracic carotid–subclavian bypass (using a prosthetic conduit) requires a brief period of complete clamp of the carotid artery for anastomosis that is usually well tolerated. An intraluminal shunt is necessary only if there are significant lesions in the contralateral common or internal carotid arteries.
- Extrathoracic subclavian transposition (subclavian to carotid anastomosis) requires more extensive dissection compared to carotid–subclavian bypass. Phrenic nerve injury or the thoracic duct injury is possible.
- Axillary-axillary bypass can be done when there is significant ipsilateral carotid disease. The prosthetic graft is usually placed underneath the skin overlying the sternum. A sternotomy after an axillary-axillary bypass would put the graft at risk.
- Subclavian endarterectomy requires thoracotomy is rarely performed.
- Postoperative monitoring:
- Bleeding in the access site
- Neurological status (cerebral ischemic events from thrombosis of the target vessel or distal embolization up the carotid or vertebral arteries)
- Check BP in both arms
- To prevent coronary–subclavian steal syndrome, it is crucial to rule out any high-grade proximal stenosis in the left subclavian artery before LIMA is considered as a graft (3). At a minimum, bilateral upper extremity noninvasive BP should be checked. A difference of 15 mm Hg identifies all patients with subclavian stenosis of >50% (4). If present, stent the subclavian artery prior to CABG, then use an in situ LIMA graft. In an emergent setting, a free LIMA graft to LAD appears to be a reasonable choice (1).
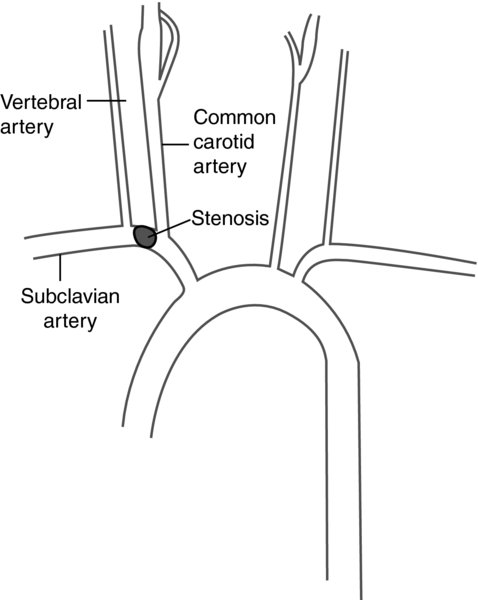
FIGURE 1. Blockage of the subclavian artery proximal to the vertebral artery.
During exercise, blood vessels in the arm dilate (decrease resistance). Blood from the cerebral vasculature flows preferentially in the direction of decreased resistance retrograde down the vertebral artery. This results in “steal”.