Bone and Soft-Tissue Disorders
= soft-tissue injury with break in continuity of bone or cartilage
General description:
- OPEN / CLOSED
open Fx = communication between fractured bone + skin - COMPLETE / INCOMPLETE
complete Fx = all cortical surfaces disrupted
incomplete Fx = partial separation of bone
Incomplete pediatric fractures:- longitudinal compressive force:
- buckle / torus Fx
- bowing Fx = plastic deformity of thin long bone (ulna >clavicle, fibula)
- force perpendicular to long axis of bone greenstick Fx
- combination fracture lead-pipe Fx = combination of greenstick + torus Fx
- longitudinal compressive force:
- SIMPLE / COMMINUTED
simple Fx = noncomminuted
comminuted Fx = >2 fragments
segmental Fx = isolated segment of shaft
butterfly fragment = V-shaped fragment not completely circumscribed by cortex - DIRECTION OF FRACTURE LINE relative to long axis of bone:
- transverse, oblique, oblique-transverse, spiral
Special terminology:
- avulsion Fx = fragment pulled off by tendon / joint capsule / ligament from parent bone
- transchondral Fx = cartilaginous surface involved
- chondral Fx = cartilage alone involved
- osteochondral Fx = cartilage + subjacent bone involved
Description of anatomic positional changes:
= change in position of distal fracture fragment in relation to proximal fracture fragment
LENGTH = longitudinal change of fragments
- distraction = increase from original anatomic length
- shortening = decrease from original anatomic length
- impacted = fragments driven into each other
- overriding = also includes latitudinal changes
- overlapping = bayonet apposition
DISPLACEMENT = latitudinal change of anatomic axis
- undisplaced
- anterior, posterior, medial / ulnar, lateral / radial
ANGULATION / TILT
= long axes of fragments intersect at the fracture apex:
- medial / lateral, ventral / dorsal
- varus = angular deviation of distal fragment toward midline on frontal projection
- valgus = angular deviation of distal fragment away from midline on frontal projection
eg, “ventral angulation of fracture apex”
eg, “in anatomic / near anatomic alignment”
ROTATION
- Difficult to detect radiographically!
- differences in diameters of apposing fragments
- mismatch of fracture line geometry
- internal / external rotation
NUC:
Typical time course:
- Acute phase (3–4 weeks) abnormal in 80% <24 hours, in 95% <72 hours
- Elderly patients show delayed appearance of positive scan
- broad area of increased tracer uptake (wider than fracture line)
- Subacute phase (2–3 months) = time of most intense tracer accumulation
- more focal increased tracer uptake corresponding to fracture line
- Chronic phase (1–2 years)
- slow decline in tracer accumulation
- in 65% normal after 1 year; >95% normal after 3 years
Return to normal:
- Non–weight-bearing bone returns to normal more quickly than weight-bearing bone
→ rib fractures return to normal most rapidly - Complicated fractures with orthopedic fixation devices take longest to return to normal
- Simple fractures: 90% normal by 2 years
- Open reduction / fixation: <50% normal by 3 years
- Delayed union: slower than normal for type of fracture
- Nonunion: persistent intense uptake in 80%
- Complicated union (true pseudarthrosis, soft-tissue interposition, impaired blood supply, presence of infection)
- intense uptake at fracture ends
- decreased uptake at fracture site
- Vertebral compression fractures: 60% normal by 1 year; 90% by 2 years; 97% by 3 years
= fracture at site of preexisting osseous abnormality
Cause: tumor, osteoporosis, infection, metabolic disorder
= fracture produced as a result of repetitive prolonged muscular action on bone exceeding its capability for self-repair
Insufficiency Fracture
= normal physiologic stress applied to bone with abnormal elastic resistance / deficient mineralization
Cause:
- Osteoporosis
- Renal osteodystrophy
Types of Fractures
Type Bone Quality Load Traumatic normal single large Fatigue (stress) normal repetitive Insufficiency (stress) abnormal (metabolic) minimal Pathologic abnormal (tumor) minimal - Osteomalacia / rickets
- Hyperparathyroidism
- Radiation therapy
- Rheumatoid arthritis
- Paget disease
- Fibrous dysplasia
- Osteogenesis imperfecta
- Osteopetrosis
- Prolonged corticosteroid treatment
- Tumor treatment with ifosfamide, methotrexate
Location: thoracic vertebra, sacrum, pubic bone, ilium, lower extremity (calcaneus, tibia, fibula)
Fracture orientation: perpendicular to long axis of bone
Plain film / CT (1–2 weeks after onset of fracture):
- often normal in early stage of fracture
- cortical linear lucency ← disruption (= fracture line)
- localized cortical thickening
- periosteal new bone formation
- medullary sclerosis (endosteal callus formation)
MR:
- zone of low SI on T1WI + variable intensity on T2WI (= discrete fracture line)
- surrounded by diffuse marrow edema (hypointense on T1WI + hyperintense on T2WI) = stress reaction
- circumferential periosteal reaction + early callus + surrounding edema adjacent to bone hyperintense on T2WI + enhancement after IV Gd-chelate (DDx: osteomyelitis with more eccentric involvement)
NUC (bone scan):
- increased abnormal uptake
Pelvic Insufficiency Stress Fracture
- severe pain in lower back + sacroiliac joints; radiates to buttocks, hips, groin, legs; worsens with weight bearing
- walking ability impaired
Prevalence: 1.8–5% of women >55 years
Predisposed: postmenopausal women
Location: sacral ala, parasymphyseal region of os pubis, pubic rami, supraacetabular region, iliac blades, superomedial portion of ilium
Types:
- occult fracture:
Site: sacrum >supraacetabulum, ilium- sclerotic band, cortical disruption, fracture line
- Often obscured by overlying bowel gas + osteopenia!
- aggressive fracture:
Site: parasymphysis, pubic rami- exuberant callus formation, osteolysis + fragments ← prolonged / delayed healing / chronic nonunion
CAVE: fracture may be misdiagnosed as neoplasm; interpretation also histologically difficult
NUC:
- butterfly / H-shaped (“Honda” sign) / asymmetric incomplete H-shaped pattern of sacral uptake
- pelvic outlet view for parasymphyseal fx
CT and MR (most accurate modalities):
- sclerotic band, linear fracture line, cortical disruption, fragmentation, displacement
- bone marrow edema
- Excludes bone destruction + soft-tissue masses!
Prognosis: healing in 12–30 months
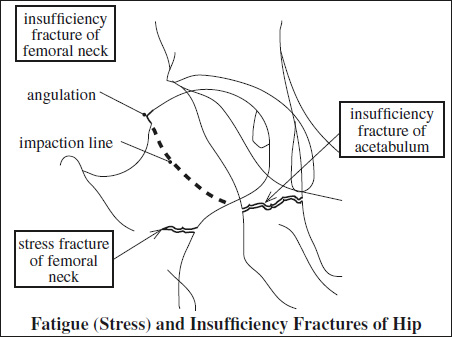
Femoral Insufficiency Fracture
Site: subcapital
- subtle femoral neck angulation
- trabecular angulation
- subcapital impaction line
Fatigue (Stress) Fracture
= normal bone subjected to repetitive stresses (none of which is singularly capable of producing a fracture) → leading to mechanical failure over time
Risk factors: new / different / rigorous repetitive activity; female sex; increased age; Caucasian race; low bone mineral density; low calcium intake; fluoride treatment for osteoporosis; condition resulting in altered gait
- activity-related pain abating with rest
- constant pain with continued activity
- infraction in the center of an area of cortical thickening
- extensive bidirectional cortical thickening from endosteum to periosteum
- focal cortical ridge
NUC:
- linear intense uptake of tracer
DDx: Osteoid osteoma (round nidus, no cortical ridge, “double-density” sign on bone scan)
- Spine
- Clay shoveler's fracture: spinous process of lower cervical / upper thoracic spine
- Spondylolysis = pars interarticularis of lumbar vertebra: ballet, gymnastics, diving
- Ribs: carrying heavy pack, golf, coughing
- Pelvis
- Obturator ring of pelvis: stooping, bowling, gymnastics
Site: superior / inferior pubic ramus - Sacrum (<2%): long-distance runner, military recruits
Site: unilateral ? ← leg length discrepancy
- Obturator ring of pelvis: stooping, bowling, gymnastics
- Upper extremity
- Clavicle: postoperative (radical neck dissection)
- Coracoid process of scapula: trap shooting
- Coronoid process of ulna: pitching ball, throwing javelin, pitchfork work, propelling wheelchairs
- Distal shaft of humerus: throwing ball (basketball, baseball, softball, javelin)
- Hook of hamate: swinging golf club / tennis racquet / baseball bat
- Other wrist bones: capitate >lunate >scaphoid
- Lower extremity
- Femur
- neck: ballet, long-distance running
Site: inferior surface of medial femoral neck- subtle lucency / sclerosis (= acute fracture)
- lucent line surrounded by sclerosis (= subacute fracture)
- shaft: ballet, marching, long-distance running, gymnastics
- distal metaphysis: endurance athlete (runner, soccer player, triathlete)
- neck: ballet, long-distance running
- Patella: hurdling
- Tibial shaft:
- proximal diaphysis: running
- middle + distal diaphysis: football, soccer, tennis, ballet, jogging
- Shin splint = early stress response
- Fibula (distal diaphysis): long-distance running, jumping, parachuting
- Femur
- Foot (in order of frequency):
- 2nd>3rd + 4th metatarsal: marching, stomping on ground, prolonged standing, ballet, long-distance running, postoperative bunionectomy
- Calcaneus: jumping, parachuting, prolonged standing, long standing, recent immobilization
- vertical / oblique fracture orientation anterior to tuberosity
- Tarsal navicular: stomping on ground, marching, long-distance running, prolonged standing, ballet
- vertically oriented fracture in midbody
- Midfoot fractures are difficult to diagnose by conventional radiography; CT + MRI are often helpful
- Sesamoids of metatarsal: prolonged standing, gymnastics, long jumping
X-RAY (15% sensitive in acute fractures, increasing to 50% on follow-up):
- cancellous (trabecular) bone (notoriously difficult to detect)
- subtle blurring of trabecular margins
- faint sclerotic radiopaque area of peritrabecular callus (50% change in bone density needed)
- sclerotic band (← trabecular compression + callus formation) usually perpendicular to cortex
- compact (cortical) bone
- “gray cortex” sign = subtle ill definition of cortex
- intracortical radiolucent striations (early)
- solid thick lamellar periosteal new bone formation
- endosteal thickening (later)
- Follow-up radiography after 2–3 weeks of conservative therapy
NUC (no longer “gold standard” compared with MR):
- Highly sensitive with low specificity + ineffective in early cortical stress injuries
- abnormal uptake within 6–72 hours of injury (prior to radiographic abnormality)
- “stress reaction” = focus of subtly increased uptake
- focal fusiform area of intense cortical uptake
- abnormal uptake persists for months
MR (very sensitive modality; fat saturation technique most sensitive as it detects an increase in water content of medullary edema / hemorrhage):
- increased marrow SI on T2WI + STIR (extensive micro- fractures cause edema + hemorrhage, which may obscure the fracture line); resolves within 6 months in 90%
- low-intensity band contiguous with cortex on T2WI = fracture line of more advanced lesion
- diminished marrow SI on T1WI of fracture line (less helpful)
- periosteal edema = hyperintense line along periosteal surface on T2WI
CT (best modality for cortical abnormalities):
helpful in: longitudinal stress fracture of tibia; in confusing pediatric stress fracture (to detect endosteal bone formation)
- cortical abnormalities:
- osteopenia = increased hypoattenuation
- resorption cavities = round / oval hypoattenuating intracortical defect
- striations = subtle hypoattenuating intracortical lines
DDx:
- Shin splints (activity not increased in angiographic / blood-pool phase)
- long linear uptake on posteromedial (soleus muscle) / anterolateral (tibialis anterior muscle) tibial cortex on delayed images (from stress to periosteum at muscle insertion site)
- Osteoid osteoma (eccentric, nidus, solid periosteal reaction, night pain)
- Chronic sclerosing osteomyelitis (dense, sclerotic, involving entire circumference, little change on serial radiographs)
- Osteomalacia (bowed long bones, looser zones, gross fractures, demineralization)
- Osteogenic sarcoma (metaphyseal, aggressive periosteal reaction)
- Ewing tumor (lytic destructive appearance with soft-tissue component, little change on serial radiographs)
Apophyseal Injury = Avulsion Fracture
Mechanism: excessive avulsive force
◊Physis under secondary ossification center is weakest part!
At risk: young athletes: hurdlers, sprinters, cheerleaders (repetitive to and fro adduction / abduction + flexion / extension)
Age: children >adults
Avulsion injury of lesser trochanter in adults suggests underlying malignant disease
- pain, point tenderness, swelling
- physeal widening
- irregularity at site of avulsion
- displaced pieces of bone of variable size:
- crescentic ossific opacity if viewed on tangent
- very subtle disk-shaped opacity if seen en face
- abnormal foci of heterotopic ossification (later)
- prominent bone formation in chronic avulsion injury from overuse with repeated microtraumas
DDx of healing acute injury: osteomyelitis, Ewing sarcoma
Little League Shoulder
= overuse injury to proximal humeral physis
Mechanism: excessive overhead throwing
Apophyseal Avulsion Injuries
|
- widening + irregularity of proximal humeral physis
Little League Elbow
= traction injury of medial humeral epicondyle
Mechanism: pitching → valgus stress of cocking and acceleration
- localized bone marrow edema
- widening of physis
Gymnast Wrist
Mechanism: repetitive weight bearing on wrist
- physeal stress changes of distal radius ± ulna
- positive ulnar variance ← abnormal distal radial growth
Cx: strain / tear of triangular fibrocartilage complex
Prevalence: 6–18–30% of bone injuries in children <16 years
Peak age: 12 years
Location: distal radius (28%), phalanges of hand (26%), distal tibia (10%), distal phalanges of foot (7%), distal humerus (7%), distal ulna (4%), proximal radius (4%), metacarpals (4%), distal fibula (3%)
Mechanism: 80% shearing force; 20% compression
Resistance to trauma: ligament >bone >physis (hypertrophic zone most vulnerable)
MR:
- focal dark linear area (= line of cleavage) within bright physis on gradient echo images (GRE)
Cx:
- progressive angular deformity from segmental arrest of germinal zone growth with formation of a bone bridge across physis = “bone bar”
- limb length discrepancy from total cessation of growth
- articular incongruity from disruption of articular surface
- Bone infarction in metaphysis / epiphysis
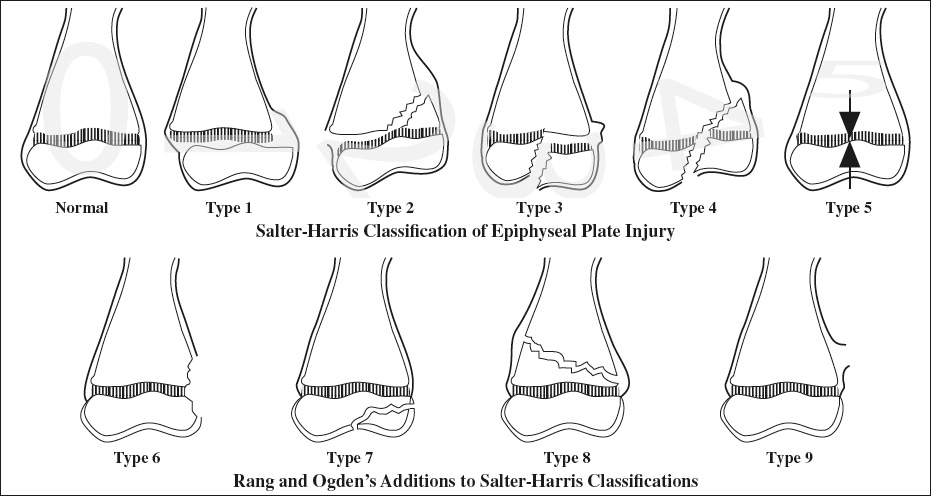
Salter-Harris Classification:
(considering probability of growth disturbance)
[Robert Bruce Salter (1924–) and W. Robert Harris (1922–), orthopedic surgeons in Toronto, Canada]
◊Prognosis is worse in lower extremities (ankle + knee) irrespective of Salter-Harris type!
mnemonic: SALTR
- S lip of physis = type 1
- A bove physis = type 2 (distal)
- L ower than physis = type 3 (proximal)
- T hrough physis = type 4
- R ammed physis = type 5
Salter Type 1 (6–8.5%)
= slip of epiphysis (← shearing force separates epiphysis from physis)
Line of cleavage: confined to physis
Location: most commonly in phalanges, distal radius (includes: apophyseal avulsion, slipped capital femoral epiphysis)
- widening of growth plate
- displacement of epiphyseal ossification center
Prognosis: favorable irrespective of location
Salter Type 2 (73–75%)
= shearing force splits growth plate
Line of fracture: through physis + extending through margin of metaphysis separating a triangular metaphyseal fragment (= “corner” sign)
Location: distal radius (33–50%), distal tibia + fibula, phalanges
Prognosis: good, may result in minimal shortening
Salter Type 3 (6.5–8%)
= intraarticular fracture, often occurring after partial closure of physis
Line of fracture: vertically / obliquely through epiphysis + extending horizontally to periphery of physis
Location: distal tibia, distal phalanx, rarely distal femur
- epiphysis split vertically
Prognosis: fair (imprecise reduction leads to alteration in linearity of articular plane)
Salter Type 4 (10–12%)
Location: lateral condyle of humerus, distal tibia
- fracture involves metaphysis + physis + epiphysis
Prognosis: guarded (may result in deformity + angulation)
Triplane Fracture (6%)
Location: distal tibia, lateral condyle of distal humerus
- vertical fracture of epiphysis + horizontal cleavage plane within physis + oblique fracture of adjacent metaphysis
Salter Type 5 (<1%)
= crush injury with injury to vascular supply
Location: distal femur, proximal tibia, distal tibia
Often associated with: fracture of adjacent shaft
- no immediate radiographic finding
- shortening of bone + cone epiphysis / angular deformity on follow-up
Prognosis: poor (impairment of growth in 100%)
Most scapular fractures are minimally displaced extraarticular fractures of the scapular body, acromion, or coracoid process. Fractures of the glenoid neck or articular surface are more likely to require surgical repair.
= rare <1% of all extremity fractures
Mechanism: high-energy chest trauma
In 90% associated with: injury to chest, spine, pelvis, internal organs, brachial plexus, axillary vessels
= may consist of up to 4 parts (fragment displaced by ≥1 cm / angled by ≥45°)
- anatomic head
- metaphyseal fragment with lesser tuberosity
- metaphyseal fragment with greater tuberosity
- humeral shaft
Prognosis: anatomic neck fractures are associated with an increased risk of avascular necrosis. The PPV is 97% if combined with a medial metaphyseal fragment <8 mm short and >2 mm displaced.
Neer classification (1970):
- 1-part fracture (85%) = no displacement / angulation
- 2- / 3- / 4-part fracture (15%)
Pediatric Elbow Fracture
Age: common at 2–14 years
- Soft-tissue
- displacement of anterior + posterior fat pads (= elbow joint effusion with supracondylar / lateral condylar / proximal ulnar fractures)
- displaced supinator fat pad (= fracture of proximal radius)
- focal edema medially (= medial epicondyle fx) / laterally (= lateral condyle fx)
- Humerus (80%)
Supracondylar fracture (55%)- Mechanism: hyperextension with vertical stress
- transverse fracture line
- distal fragment posteriorly displaced / tilted
- anterior humeral line intersecting anterior to posterior third of capitellum (on lateral x-ray)
Lateral condylar fracture (20%)- Mechanism: hyperextension with varus stress
- fracture line between lateral condyle + trochlea / through capitellum
Medial epicondylar fracture (5%)- Mechanism: hyperextension with valgus stress
- avulsion of medial epicondyle (by flexor muscles of forearm)
- may become trapped in joint space (after reduction of concomitant elbow dislocation)
- Radius (10%)
Mechanism: hyperextension with valgus stress- Salter-Harris type II / IV fracture
- transverse metaphyseal / radial neck fracture
Mechanism: hyperextension with varus stress- dislocation as part of Monteggia fracture (from rupture of annular ligament)
- Ulna (10%)
- longitudinal linear fracture through proximal shaft
Mechanism: hyperextension with vertical stress
- transverse fracture through olecranon
Mechanism: hyperextension with valgus / varus stress; blow to posterior elbow in flexed position - coronoid process avulsion
Mechanism: hyperextension-rotation associated with forceful contraction of brachial m.
- longitudinal linear fracture through proximal shaft
2nd most common joint dislocation in adult after shoulder
- Posterior elbow dislocation
- Anterior dislocation (rare): most often in child as a result of rebound following posterior dislocation
Associated soft-tissue injury (in sequence): lateral → medial
- Lateral collateral ligament complex
- Joint capsule + other lateral structures
- MCL complex
Associated osseous injury:
- Fracture of radial head + coronoid process (= terrible triad); medial epicondyle fracture; Essex-Lopresti fracture (rare)
Pediatric Distal Forearm Fracture
Buckle / Torus Fracture
= break in soft fibrous cortex with frequently intact periosteal sleeve
Cause: longitudinal compressive force
Location: distal radial + ulnar metaphyses
- buckle in cortex on compression side of fracture
- intact cortex on tension side
Prognosis: excellent stability; healing without complications after cast / splint immobilization
Greenstick Fracture
= break of bone cortex on tension side + intact periosteum
Cause: force perpendicular to long axis of bone
- cortical disruption on tension (convex) side of fracture
- intact cortex on compression side
Prognosis: unstable fracture → continued displacement for first 2 weeks
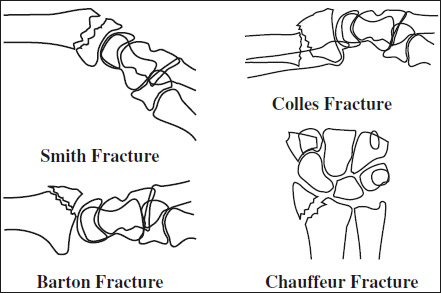
Barton Fracture
[John Rhea Barton (1794–1871), orthopedic surgeon at Pennsylvania Hospital, Philadelphia]
Mechanism: fall on outstretched hand
- intraarticular oblique fracture of ventral / dorsal lip of distal radius
- carpus dislocates with distal fragment up + back on radius
Chauffeur Fracture
= HUTCHINSON FRACTURE = BACKFIRE FRACTURE = LORRY DRIVER FRACTURE
[Jonathan Hutchinson (1828–1913), British surgeon]
= name derived from direct trauma to radial side of wrist sustained from recoil of crank used in era of hand cranking to start automobiles
Mechanism: acute dorsiflexion + abduction of hand
- triangular fracture of radial styloid process
Colles Fracture
[Abraham Colles (1773–1843), surgeon in Dublin, Ireland]
= POUTEAU FRACTURE (term used in France)
[Claude Pouteau (1725–1775), surgeon in Lyon, France]
◊Most common fracture of forearm!
Mechanism: fall on outstretched hand
- nonarticular radial fracture in distal 2 cm
- dorsal displacement of distal fragment + volar angulation of fracture apex
- ± ulnar styloid fracture
- “silver-fork” deformity
Cx: posttraumatic arthritis
Rx: anatomic reduction important
Significant postreduction deformity:
- Residual positive ulnar variance >5 mm indicates unsatisfactory outcome in 40%
- Dorsal angulation of palmar tilt >15° decreases grip strength + endurance in >50%
Essex-Lopresti Fracture
[Peter Gordon Essex-Lopresti (1918–1951), surgeon at Birmingham Accident Center, England]
Mechanism: FOOSH-type injury
- wrist pain / tenderness
- “floating radius”:
- comminuted displaced radial head fracture
- dislocation of distal radioulnar joint = discrepancy of radioulnar distance >5 mm compared to contralateral uninjured wrist (on lateral radiograph)
- disruption of interosseous membrane
Rx: nearly always surgical intervention
Galeazzi Fracture
[Ricardo Galeazzi (1866–1952), orthopedic surgeon in Italy]
= PIEDMONT FRACTURE
Mechanism: fall on outstretched hand with elbow flexed
- radial shaft fracture (most commonly) at junction of distal to middle third with dorsal angulation
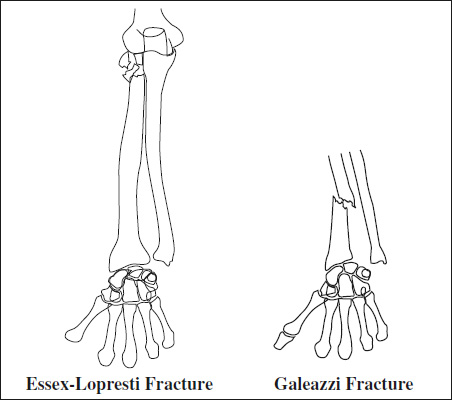
- subluxation / dislocation of distal radioulnar joint
- ulnar plus variance (= radial shortening) of >10 mm implies complete disruption of interosseous membrane = complete instability of radioulnar joint
Cx:
- High incidence of nonunion, delayed union, malunion (unstable fracture)
- Limitation of pronation / supination
Galeazzi-equivalent Fracture
= exclusively in skeletally immature children
Mechanism: hyperpronation / hypersupination
- radial shaft fracture (4 primary types)
- dislocation / epiphyseolysis of distal ulna
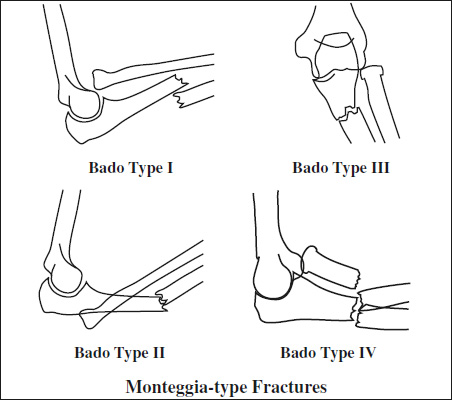
Monteggia-type Fracture
= ulnar shaft fracture + (often missed) radiocapitellar dislocation
Bado Classification:
[Jose Luis Bado (1903–1977), orthopedic surgeon in Uruguay]
Type I = classic Monteggia fracture
[Giovanni Battista Monteggia (1762–1815), professor of anatomy and surgery at Istituzioni Chirurgiche at University of Pavia]
Mechanism: direct blow to the forearm
- anteriorly angulated proximal ulnar fracture
- anterior dislocation of radial head
- may have associated wrist injury
Cx: nonunion, limitation of motion at elbow, nerve abnormalities
Type II = reverse Monteggia fracture
- radial head displaced posteriorly / posterolaterally
- dorsally angulated proximal ulnar fracture
Type III
- lateral dislocation of radial head
- ulnar metaphyseal fracture
Type IV
- anterior displacement of radial head
- fracture of proximal third of radius + ulna at the same level
Smith Fracture
= REVERSE COLLES FRACTURE = REVERSE BARTON FRACTURE = GOYRAND FRACTURE (term used in France)
[Robert William Smith (1807–1873), succeeding Colles as professor of surgery at Trinity College in Dublin, Ireland]
Mechanism: hyperflexion with fall on back of hand
- nonarticular distal radial fracture
- ventral displacement of fragment
- radial deviation of hand
- “garden spade” deformity
Cx: altered function of carpus
Hamate Fracture
Prevalence: 1.7% of all carpal fractures
Mechanism: handle of racket / bat / club presses against protruding hook; axial loading force on body with clenched fist; fall on outstretched hand
May be associated with: perilunate dislocation
Location:
- hamate hook at palmar nonarticular surface
- body
- grip weakness; pain with resistance to flexion of 5th finger
- hamulus not depicted on standard PA view
- cortical density of hamulus lower than normal
Cx: 5th finger flexor tendon rupture; ulnar nerve palsy; hook nonunion
DDx: os hamuli proprium (ovoid / pyramidal bone with peripheral cortical bone)
Rx: open reduction with internal fixation for fractures displaced >1 mm
Lunate Fracture
Prevalence: 4% of all carpal fractures
Mechanism: direct axial compression from head of capitate driven into lunate
Location: volar pole; dorsal pole; body
Fracture orientation: transverse, sagittal
Cx: nonunion → Kienböck disease
Pisiform Fracture
Prevalence: 1.3% of all carpal fractures (only 50% are diagnosed on PA radiograph)
Mechanism: fall on outstretched hand with direct impact on pisiform bone
May be associated with: carpal dislocation, distal radial fracture
Fracture type: linear, comminuted, chip
Cx: ulnar nerve injury
Rx: excision of pisiform bone
Scaphoid Fracture
= NAVICULAR FRACTURE
◊Most frequent (90%) of all carpal bones fractures!
Age: active men during 2nd + 3rd decade
Mechanism: fall on dorsiflexed outstretched hand (hyperextension injury)
Location: waist (80%) >proximal pole
Fracture orientation: horizontal oblique, vertical oblique, transverse
- pain + tenderness at anatomic snuff box
Radiographic misses: 25–33–65%
N.B.: If initial radiograph negative, reexamine in 2 + 6 weeks after treatment with thumb-spica cast or proceed to CT / MRI!
CT: 89–97% sensitive; 85–100% specific; 97–99% NPV; 6–12 seconds examination time
MR: high sensitivity; 30–40 minutes examination time
Bone scan: up to 100% sensitive, 93% PPV after 2–3 days
Prognosis: dependent on following factors
- fracture displacement with >1 mm offset / angulation / rotation of fragments (less favorable)
- location of blood supply:
- distal ⅓ (10%) = usually fragments reunite
- middle ⅓ (70%) = failure to reunite in 30%
- proximal ⅓ (20%) = failure to reunite in 90%
- orientation of fracture
- transverse / horizontal oblique = relatively stable
- vertical oblique (less common) = unstable
- Good prognosis with distal fracture + no displacement + no ligamentous injury!
- Less favorable prognosis with displaced / comminuted fracture + proximal pole fracture!
Cx:
- Malunion; delayed union; nonunion (5–15%)
- Progressive fragment displacement
- Avascular necrosis of proximal fragment (13–50%); higher prevalence if proximal pole fractured ← distal location of main nutrient a.
Trapezium Fracture
Prevalence: 3–5% of all carpal fractures
Mechanism: direct blow to volar surface / avulsion
Location: trapezial ridge (= vertical prominence on volar aspect); body
Associated with: carpometacarpal joint involvement; fracture through base of 1st metacarpal / scaphoid
Triquetral Fracture
Prevalence: 18% of all carpal fractures
Mechanism: wrist hyperextension with ulnar deviation → impingement of ulnar styloid process against dorsal surface of triquetrum
Location:
- dorsal ridge fracture
- triquetral body fracture (in combination with perilunate dislocation)
- fragment along dorsal edge of triquetrum (LAT view in slight pronation)
Bennett Fracture
[Edward Halloran Bennett (1837–1907), surgeon in Dublin, Ireland]
Mechanism: forced abduction of thumb
- intraarticular fracture-dislocation of base of 1st metacarpal
- small fragment of 1st metacarpal continues to articulate with trapezium
- lateral retraction of 1st metacarpal shaft by abductor pollicis longus
Rx: anatomic reduction important, difficult to keep in anatomic alignment
Cx: pseudarthrosis
Boxer's Fracture
Mechanism: direct blow with clenched fist
- transverse fracture of distal metacarpal (usually 5th)
Gamekeeper's Thumb
= SKIER'S THUMB (originally described as chronic lesion in hunters strangling rabbits)
Frequency: 6% of all skiing injuries; 50% of skiing injuries to the hand
Mechanism: violent abduction of thumb with injury to ulnar collateral ligament (UCL) in 1st MCP (faulty handling of ski pole)
- disruption of ulnar collateral ligament of 1st MCP joint, usually occurring distally near insertion on proximal phalanx
- avulsed bone fragment (in 12% of lesions)
- radial stress examination results in abduction angle >35–45° or >10° greater than on opposite side
- Controversial maneuver to document ligamentous disruption as it may complete incomplete tear
- displacement of UCL superficial to aponeurosis of adductor pollicis (= Stener lesion) [torn end of UCL may be marked by avulsed bone fragment]
Rolando Fracture
[Silvio Rolando (?–1931?), surgeon in Genoa, Italy]
- comminuted Y- / T-shaped intraarticular fracture-dislocation through base of thumb metacarpal
Prognosis: worse than Bennett fracture (difficult to reduce)
Rib Fracture
◊Most common skeletal injury in blunt chest trauma (in 50%)
Associated with: pneumothorax, hemothorax, lung contusion / laceration
CT is the most sensitive technique for imaging rib fractures by determining the site and number of fractures and providing information about any associated injuries.
- 1st–3rd rib
◊ Indicates high-energy trauma ← protected location
Cause: acute trauma / fatigue fracture (from carrying a heavy back pack)
Associated with: aortic / great vessel + subclavian vascular injury; brachial plexus injury; thoracic vertebral fracture; scapular fracture - Lower ribs
Associated with: injury to liver, spleen, kidney, diaphragm
Cx: atelectasis + subsequent pneumonia ← limited respiratory movement
Flail Chest
= segmental fracture of >3 contiguous ribs in >2 places
In >50% associated with: significant intrathoracic injury that requires surgical Rx
- paradoxic motion of fractured chest wall with respiration on clinical examination
- respiratory failure
Rx: mechanical ventilation for prolonged periods
Cough Fracture
Location: 4th–9th rib in anterior axillary line
Scapula Fracture
Prevalence: 3–5% of all shoulder girdle fractures
- In 3.7% of patients with multiple injuries
Cause: motor vehicle accident, fall from great height
Associated with: pneumothorax, hemothorax, lung injury, spinal injury (in 35–98%)
Prognosis: displaced glenoid intraarticular fracture + displaced juxtaarticular fracture require surgical management
Sternal Fracture
Cause: deceleration, direct blow
Associated with: anterior mediastinal hemorrhage
Sternal fractures are best demonstrated on multiplanar reformatted CT images, especially on sagittal views.
Unstable pelvic fractures:
- anterior compression
- Bilateral vertical pubic rami fractures
- Symphysis + sacroiliac joint diastasis
- lateral compression
- Malgaigne (ipsilateral anterior + posterior fx)
- Bucket-handle (contralateral anterior + posterior fx)
- vertical shear
- Superior displacement of pelvis
Acetabular Fracture
Anatomy & Function:
most important portion of acetabulum is roof / dome; weight-bearing surface for entire lower limb is derived + supported by 2 columns which are oriented in an inverted “Y” and join above the acetabular roof at an angle of 60°:
- anterior iliopubic column of acetabulum
- posterior ilioischial column of acetabulum
Classification (Judet and Letournel):
- Elementary 5 fractures
Posterior wall* 27% Anterior column 5%
Transverse* 9% Posterior column 4%
Anterior wall 2% - Associated 5 fractures (= combinations / partial combinations of elementary fractures)
Transverse + posterior wall* 27%
Both columns* 19%
T-shaped* 6%
Anterior wall + posterior hemitransverse 5%
Posterior column + posterior wall 3%
*= account for 80%of all acetabular fractures (3 most common types underlined)
Posterior wall (lip / rim) fracture (27%)
Mechanism: indirect force transmitted through length of femur with flexed hip joint (knee strikes dashboard)
Associated with: posterior dislocation of femur
A posterior wall fracture involves only the posterior articular surface and is not seen on the medial acetabular surface.
Transverse fracture (9%)
N.B.: most difficult to diagnose + comprehend
- transects both the iliopubic + ilioischial columns with fracture line in an anteroposterior direction
On subsequent axial CT images, a transverse acetabular fracture is represented by a sagittal fracture line simulating anterior and posterior wall fractures, a pitfall easily avoided with 3-D reconstructions.
Anterior column fracture (5%)
Mechanism: blow to greater trochanter with hip externally rotated
Associated with: posterior column / transverse fracture
- fracture begins between anterior iliac spines + traverses the acetabular fossa + ends in the ischiopubic ramus
Posterior column fracture (4%)
Mechanism: indirect force transmitted through length of femur with hip abducted
Associated with: posterior dislocation of femur + sciatic nerve injury
- fracture begins at greater sciatic notch + traverses the posterior aspect of acetabular fossa + ends in the ischiopubic ramus
Anterior wall fracture (2%)
Mechanism: force transmitted through greater trochanter

Associated with: posterior dislocation of femur + sciatic nerve injury
- fracture begins on anterior rim of acetabulum + emerges on lateral aspect of superior pubic ramus
Associated Both Column fracture (19%)
= separation of both columns from each other with 2 dominant fractures nearly perpendicular to each other
Associated with: additional fracture lines + medial displacement of femoral head
- “spur sign” = shard of bone superior to femoral neck (on obturator view)
With both-column fractures the entire weight-bearing portion of the acetabulum is disconnected from the sciatic buttress.
Bucket Handle Fracture
- double vertical fracture through superior and inferior pubic rami + sacroiliac joint dislocation on contralateral side
Duverney Fracture
[Joseph Guichard Duverney (1648–1730), French surgeon]
- isolated fracture of iliac wing
Malgaigne Fracture
[Joseph François Malgaigne (1806–1865), French surgical historian, published first comprehensive book on fractures]
= fracture-dislocation of one side of the pelvis with anterior + posterior disruption of pelvic ring
Mechanism: direct trauma
- shortening of involved extremity
- vertical fractures through one side of pelvic ring
- superior to acetabulum (ilium)
- inferior to acetabulum (pubic rami)
- ± sacroiliac dislocation / fracture
- lateral unstable fragment contains acetabulum
Intracapsular Femur Fracture
- Complete Femoral Head Fracture (uncommon)
Often associated with: posterior hip dislocation
Pipkin classification:- Type 1 below fovea centralis
- Type 2 above fovea centralis with ligamentum teres often attached to fracture fragment
- Type 3 type 1/2 + femoral neck fracture
- Type 4 type 1/2 + acetabular fracture
The lateral margin of the femoral head-neck junction is crucial as it is the most common penetration point of the lateral epiphyseal vessels. Fractures involving this area create a high risk of critical vascular injury resulting in nonunion / AVN, with decreasing risk as fractures occur more distally along the femoral neck. - Osteochondral Impaction Fracture of Femoral Head
Often associated with: anterior hip dislocation- radiographically relatively occult:
- subtle flattening / focal compression defect of head
- subchondral fracture line + marrow edema at MRI
- radiographically relatively occult:
- Femoral Neck Fracture
Location: subcapital, transcervical, basicervical- valgus-impacted / nondisplaced
N.B.: frequently missed on initial radiographs ← subtlety of cortical distortion at femoral head-neck junction + only mild fracture angulation - varus-impacted (“mushroom cap” = medially rotated head) / displaced → high risk for AVN
- valgus-impacted / nondisplaced
- Femoral Neck Stress Fracture
- often initially radiographically occult
- Inferomedial cortex = fatigue fracture
Age: young athletic patient- cortical thickening + incomplete fracture line
- extensive marrow edema
- Superolateral cortex = insufficiency / fatigue fracture
Age: osteoporotic elderly- frequently displaced ← side of high tension
Extracapsular Fracture
- Intertrochanteric Fracture
Cause: frequently osteoporosis in the elderly woman
N.B.: Isolated fractures of the lesser trochanter in adults should be considered PATHOGNOMONIC for tumor infiltration. - Subtrochanteric Fracture
- comminuted / spiral morphology
Anterior Cruciate Ligament Avulsion Fracture
Age: children >adults
Mechanism:
- children: forced flexion of knee + internal rotation
- adults: severe hyperextension
May be associated with: kissing bone contusion + tear of medial collateral lig. + PCL
- aching flexed knee; signs of anterior instability
- avulsion of ACL from its distal insertion site just medial and anterior to tibial eminence
Arcuate Complex Avulsion Fracture
Mechanism: direct blow to anteromedial tibia with knee in extension / varus force to externally rotated tibia / sudden hyperextension
May be associated with:
- disruption of ACL and PCL, lateral capsular lig., iliotibial band, popliteal muscle, menisci, damage to peroneal nerve
- subtle physical finding
- mild swelling + tenderness
- “arcuate” sign = avulsed elliptic bone fragment at fibular styloid process with its long axis horizontally oriented (AP view)
- bone marrow edema in head of fibula + adjacent soft-tissue swelling
Biceps Femoris Tendon Avulsion Fracture
May be associated with:
- disruption of lateral collateral lig., Segond fracture, damage to popliteal musculotendinous unit
- irregular bone fragment off lateral fibular head in posterolateral aspect of knee joint (DDx: “arcuate sign” = horizontally oriented elliptic fragment off fibular styloid process)
- avulsion + retraction of biceps femoris tendon
Iliotibial Band Avulsion Fracture
= primary stabilizing structure of anterolateral knee
Mechanism: pure varus force (rare)
May be associated with: ACL injury
- avulsion + retraction of iliotibial band from its distal insertion on Gerdy tubercle
Posterior Cruciate Ligament Avulsion Fracture
Location: at tibial insertion site (40–55%)
Mechanism: direct blow to anterior tibia with flexed knee (dashboard injury); severe hyperextension
May be associated with:
- disruption of medial / lateral collateral ligament complexes; medial / lateral meniscal tear; bone contusion of anterior tibia + lateral femoral condyle
- focal discontinuity of posterior articular surface (LAT view)
Quadriceps Tendon Avulsion Fracture
Cause: strong deceleration in young athletes
Mechanism: sudden contraction of quadriceps muscle during jumping / kicking
- comminuted bone fragments off superior aspect of patella (LAT view)
- patella baja deformity = abnormally low position of patella with respect to femur
- marrow edema in upper pole of patella
- suprapatellar joint effusion
DDx: rupture of quadriceps tendon (at musculotendinous junction; repetitive microtrauma / systemic diseases like HPT, diabetes, collagen vascular disease, gout)
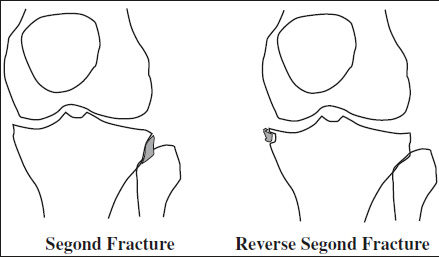
Reverse Segond Fracture
= cortical avulsion of tibial insertion of deep capsular component of medial collateral ligament
Mechanism: external rotation + valgus stress
May be associated with:
- midsubstance tear of posterior cruciate ligament; avulsion of PCL from posterior tibial plateau; tear of medial meniscus
- elliptic bone fragment arising from medial aspect of proximal tibia
Segond Fracture
[Paul Ferdinand Segond (1851–1912), surgeon in chief at Salpêtrière in Paris, France]
= cortical avulsion of the tibial insertion of middle third of lateral capsular ligament ± avulsion of iliotibial tract ± anterior oblique band
Mechanism: internal rotation + varus stress
May be associated with:
- lesion of anterior cruciate ligament (75–100%), meniscal tear (67%), avulsion of fibular attachment of long head of biceps femoris tendon + fibular collateral ligament
- pain at lateral joint line
- anterolateral rotational instability of the knee
- “lateral capsular” sign = small elliptic fragment of proximal lateral tibial rim just distal to lateral plateau parallel to tibia (AP view)
- marrow edema on MRI
Semimembranosus Tendon Avulsion Fracture
Mechanism: external rotation + abduction of flexed knee; varus force applied to flexed knee; valgus force applied to tibia
May be associated with:
- ACL tear; tear of posterior horn of medial meniscus; posterior meniscocapsular separation
- tiny avulsed bone fragment off tibia displaced posterosuperiorly (difficult to see on LAT view)
Tibial Plateau Fracture (Schatzker classification)
Type I = wedge-shaped pure cleavage fracture 6%
- <4 mm depression / displacement
- ± distraction injury to MCL / ACL
Type II = combined cleavage + lateral plateau compression fracture 25%
- distraction injury of MCL / medial meniscus in 20%
Type III = pure compression fracture of lateral tibial plateau 36%
- depression of articular surface:
- lateral depression (type IIIA)
- central depression (type IIIB)
Type IV = medial plateau fracture with a split / depressed comminution 10%
- ± distraction injury of lateral knee with LCL tear / posterolateral corner injury
- ± fracture / dislocation of proximal fibula
Cx: injury to peroneal nerve / popliteal vessels
Type V = wedge fracture of medial + lateral plateau in 3%
- often inverted Y appearance
- articular depression typically of lateral tibial plateau
- ± fracture of intercondylar eminence (= unstable 4-part fracture)
- peripheral meniscal detachment (50%)
- ACL avulsion injury (33%)
Type VI = transverse / oblique fracture with dissociation of metaphysis from diaphysis 20%
- open fracture in (33%)
◊Lateral plateau fractures (type I–III) are most common!

◊Fractures of medial plateau are associated with greater violence and higher percentage of associated injuries!
Mechanism:
- for type I + II + III = valgus force combined with axial loading (“bumper / fender fracture” from lateral force of automobile against a pedestrian's fixed knee) / compression force often on extended knee
- for type IV = varus force combined with axial loading on hyperflexed knee
- type V + VI = combination of valgus + varus stresses combined with axial loading
Tibial Tubercle Fracture
Ogden classification:
- Type 1: involvement of distal portion of tubercle
- 1A: without displacement
- 2A: with displacement
- Type 2: involvement of entire ossification center
- 2A: separation of tubercle from proximal tibia
- 2B: comminuted fracture
- Type 3: involvement of proximal tibial epiphysis into joint space
- 3A: without displacement
- 3B: with displacement
= CHILDHOOD ACCIDENTAL SPIRAL TIBIAL FRACTURE (CAST)
= lower extremity fracture associated with onset of ambulation
Cause: low-energy trauma ± rotational component
Age: toddler (9 months–3 years), young child (<8 years)
- refusal to bear weight without recognized trauma
Location: distal third to distal half of tibia; fibula, tarsus (posterior calcaneus >base of cuboid >talus)
- (typically) nondisplaced oblique spiral fracture of distal tibia
- undisplaced spiral fracture
Ankle Fracture
Frequency: ankle injuries account for 10% of all emergency room visits; 85% of all ankle sprains involve lateral ligaments
Lateral Malleolar Fractures
Weber Type A
[Bernhard Georg Weber (1929–), orthopedic surgeon in St. Gall, Switzerland]
= SUPINATION-ADDUCTION INJURY = INVERSION-ADDUCTION INJURY
Mechanism:
- avulsive forces affect lateral ankle structures
- impactive forces ← talar shift stresses medial structures
- sprain / rupture of lateral collateral ligament
- Anterior tibiofibular ligament ruptures alone in 66%
- Injury of all 3 lateral ligaments in 20%
Prognosis: chronic lateral ankle instability in 10–20%
- transverse avulsion of malleolus sparing tibiofibular ligaments
- ± oblique fracture of medial malleolus
- ± posterior tibial lip fracture
Weber Type B
= SUPINATION-ABDUCTION INJURY = EVERSION-EXTERNAL ROTATION
Mechanism:
- avulsive forces on medial structures
- impacting forces on lateral structures (talar impact)
- oblique / spiral fracture of lateral malleolus starting at level of joint space extending proximally
- lateral subluxation of talus
- partial disruption of tibiofibular ligament
- ± sprain / rupture / avulsion of deltoid ligament
- ± transverse fracture of medial malleolus
- Dupuytren Fracture
[Guillaume Dupuytren (1777–1835), French surgeon]- fracture of distal fibula above a disrupted tibiofibular ligament + disruption of deltoid lig.
- Le Fort Fracture of Ankle
[Léon Clément Le Fort (1829–1893), French surgeon]- vertical fracture of anterior medial portion of distal fibula
- avulsion of anterior tibiofibular ligament
Weber Type C
= PRONATION-EXTERNAL ROTATION = EVERSION + EXTERNAL ROTATION
- fibular fracture higher than ankle joint (Maisonneuve fracture if around knee)
- ± deltoid ligament tear
- ± medial malleolar fracture
- tear of tibiofibular ligament / avulsion of anterior tubercle (Tillaux-Chaput) / avulsion of posterior tubercle (Volkmann)
- tear of interosseous membrane = lateral instability
- Tillaux Fracture
[Paul Jules Tillaux (1834–1904), French surgeon and anatomist]- avulsion injury of anterior tibial tubercle at attachment of distal anterior tibiofibular ligament
- type 3 epiphyseal plate injury in children
- CT more sensitive in identification of fracture displacement >2 mm (cutoff that requires reduction)
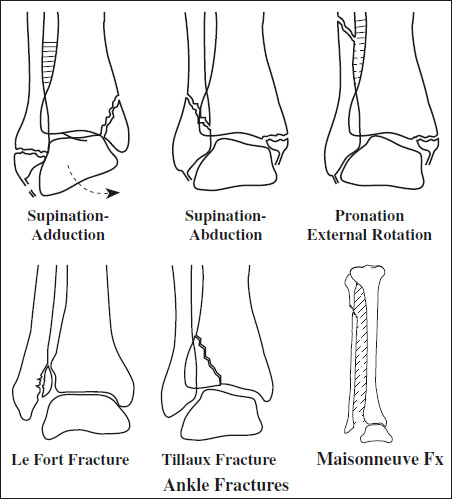
- Maisonneuve Fracture
[Jacques Gilles Maisonneuve (1809–1897), student of Dupuytren]- tear of distal tibiofibular syndesmosis + interosseous membrane
- spiral fracture of upper third of fibula
- associated fracture of medial malleolus / rupture of deep deltoid ligament
Calcaneal Fracture
Frequency: most commonly fractured tarsal bone; 60% of all tarsal fractures; 2% of all fractures in the body; commonly bilateral
Mechanism: fall from heights (axial overload)
In 10% associated with: thoracolumbar compression fracture
Age: 95% in adults, 5% in children
- adulthood: intraarticular (75%), extraarticular (25%)
- childhood: extraarticular (63–92%)
Classification:
- extraarticular fracture (25%) = no involvement of posterior talar facet:
- anterior process fracture
- fracture of mid calcaneus (body, sustentaculum tali, peroneal tubercle, lateral calcaneal process)
- fracture of posterior calcaneus (tuberosity, medial calcaneal tubercle)
- intraarticular fracture (75%)
- subtalar joint involvement: undisplaced, displaced, comminuted
- calcaneocuboid joint involvement
Sanders Classification of intraarticular fractures (correlates with prognosis):
Technique: CT with image reformation parallel + per-pendicular to posterior facet of subtalar joint
- Type I nondisplaced (<2 mm) fracture
- Type II 2 articular fragments
- Type IIA laterally located fracture line
- Type IIB centrally located fracture line
- Type IIC medially located fracture line
- Type III 3 articular fragments
- Type IIIAB lateral+ central fracture line
- Type IIIAC lateral + medial fracture line
- Type IIIBC central + medial fracture line
- Type IV >3 intraarticular fracture lines
- apex of lateral talar process does not point to “crucial angle” of Gissane
- Böhler angle decreased below 28°–40°
Chopart Fracture
[François Chopart (1743–1795), surgeon in Paris, France]
- fracture-dislocation through midtarsal / Chopart (calcaneocuboid + talonavicular) joint
- commonly associated with fractures of the bones abutting the joint
Jones Fracture
[Robert Jones (1857–1933), British orthopedic surgeon and pioneer in radiology described fracture in Ann Surg 1902]
Mechanism: adduction of forefoot with ankle in plantar flexion
- transverse fracture at base of 5th metatarsal bone at junction of diaphysis and metaphysis (>1.5 cm distal to proximal tip of metatarsal tuberosity)
Cx: delayed union / nonunion (poor blood supply)
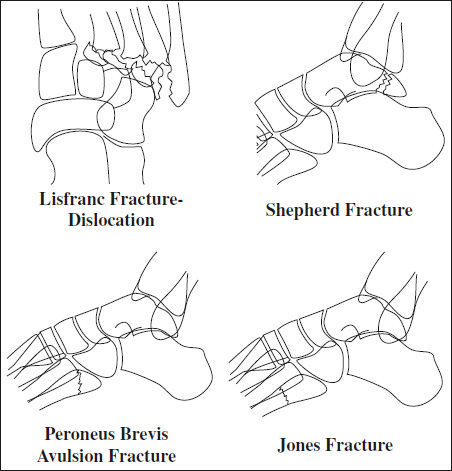
Lisfranc Fracture
[Jacques Lisfranc de Saint Martin (1787–1847), field surgeon in Napoleon's army]
Mechanism: metatarsal heads fixed and hindfoot forced plantarward and into rotation
- fracture-dislocation / fracture-subluxation of tarsometatarsal joints (typically 2 through 5)
- lateral displacement of metatarsals
Peroneus Brevis Avulsion Fracture
= METATARSAL 5 TUBEROSITY FRACTURE
◊Most common fracture of the proximal 5th metatarsal bone
Mechanism: plantar flexion + inversion (stepping off a curb)
- transverse avulsion fracture of base of 5th metatarsal bone
Location: proximal to metatarsal tuberosity (insertion of peroneus brevis tendon); usually extraarticular
DDx: Jones fracture (slightly different location)
Shepherd Fracture
[Francis J. Shepherd (1851–1929), demonstrator in anatomy at McGill University in Montreal, Canada]
- fracture of lateral tubercle of posterior process of talus
DDx: os trigonum
- Pathologic Fracture
- Stress Injury (Fracture)
- Apophyseal Injury = Avulsion Fracture
- Overuse Injury to Physis
- Epiphyseal Plate Injury
- Scapula Fracture
- Proximal Humerus Fracture
- Elbow Fracture
- Elbow Dislocation
- Forearm Fracture
- Carpal Injury
- Hand Fracture
- Chest Wall Fracture
- Pelvic Fracture
- Proximal Femur Fracture
- Knee Fracture
- Toddler's Fracture
- Foot Fracture