Anatomy and Metabolism of Bone
Normal anatomic variants can cause compression with an increased incidence of rotator cuff tears with type II and type III acromions according to cadaveric studies
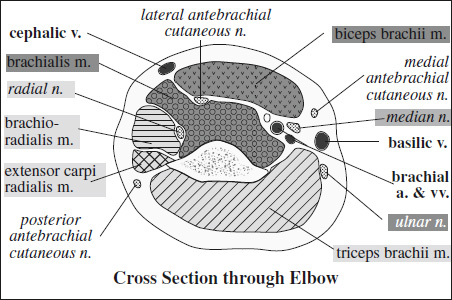
= mixed motor and sensory peripheral nerve
Origin: upper trunk of brachial plexus (roots of C5 and C6, variably from C4)
Course: deep to omohyoid m. and trapezius m. → suprascapular notch (beneath superior transverse scapular ligament) → supraspinatus fossa → around scapular spine → spinoglenoid notch→ infraspinatus fossa
Innervation:
- supraspinatus m. (motor); glenohumeral joint + acromioclavicular joint + rotator cuff + posterior ⅔ of joint capsule (sensory)
- infraspinatus m. (motor)
mnemonic: SITS
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
= 4-mm–wide triangular fibrocartilaginous rim (= extension of the glenoid fossa) with considerable variation in shape
Function: stabilizes glenohumeral joint by deepening and increasing surface area of glenoid fossa and providing attachment for glenohumeral ligaments and tendon of long head of biceps
- low SI on all pulse sequences; susceptible to magic angle artifact at 55°
- variations in attachment above epiphyseal line (= junction of upper + middle thirds of glenoid body fossa): limited to sector from 11 to 3 o'clock (anterior = 3 o'clock, posterior 9 o'clock, superior 12 o'clock, inferior 6 o'clock):






Muscle Attachments of Shoulder
Name of Muscle Origin Insertion Deltoid lateral third of clavicle deltoid tuberosity of humerus lateral border of acromion deltoid tuberosity of humerus lower part of spinous process of scapula deltoid tuberosity of humerus Subscapularis medial ⅔ of costal surface of scapula superior aspect of lesser tubercle of humerus Pectoralis major › clavicular portion medial half of clavicle crest of greater tubercle of humerus › sternocostal portion manubrium + corpus of sternum crest of greater tubercle of humerus › abdominal portion anterior sheath of rectus abdominis crest of greater tubercle of humerus Pectoralis minor 2nd / 3rd–5th ribs superomedial aspect of coracoid process Biceps brachii › long head supraglenoid tubercle of scapula tuberosity of radius › short head tip of coracoid process tuberosity of radius Coracobrachialis tip of coracoid process medial surface of middle third of humerus Supraspinatus supraspinatus fossa of scapula greater tubercle of humerus, highest facet Infraspinatus infraspinatus fossa of scapula greater tubercle of humerus, middle facet Teres minor upper ⅔ of lateral border of scapula greater tubercle of humerus, lower facet Teres major dorsum of inferior angle of scapula inferior crest of lesser tubercle of humerus - occasionally partially deficient anterosuperiorly
- labrum continuous with glenoid articular cartilage inferior to epiphyseal line
- triangular / rounded shape on cross-sectional image:
- round / cleaved / flat larger anterior labrum
- flat / round smaller posterior labrum
- blends superiorly with biceps tendon
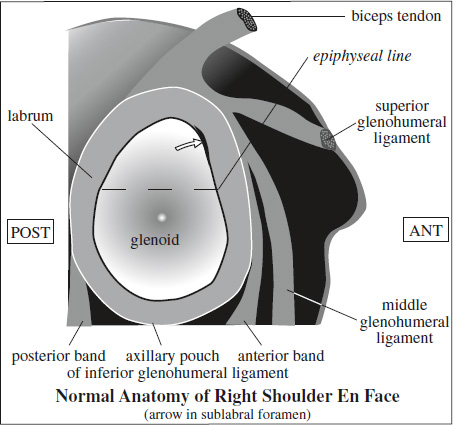
Superior Sublabral Sulcus / Recess
= variations in depth of sulcus between osseous glenoid rim + labrum
Location: 12 o'clock position at the site of biceps tendon attachment (in sagittal plane); NOT posterior to labral attachment of long head of biceps
Size: consistently 1–2 mm wide throughout its length
Types of attachment of biceps-labral complex (BLC):
- BLC firmly adherent to superior pole of glenoid without sulcus / sublabral foramen
- small sulcus = BLC attached several mm medially; hyaline cartilage beneath labrum; may be continuous with sublabral foramen which is anterior to BLC
- deep probe-patent sulcus = meniscoid labrum with large sulcus between labrum and hyaline cartilage
- may be continuous with sublabral foramen
- best visualized on oblique coronal CT / MR
DDx: type II SLAP lesion (more lateral in oblique coronal plane)
= muscle with 2 separate origins
Short Head of Biceps Brachii Muscle
- Function: ineffectual elevator of the arm
- Origin: apex of coracoid process (together with coracobrachialis tendon)
- Course: extraarticular
- Insertion: radial tuberosity (conjoined distal tendon of the short and long head)
Long Head of Biceps Brachii Muscle
- Function: ineffectual elevator of the arm
- Origin: supraglenoid tubercle of scapula ± posterosuperior glenoid labrum
- Course: traverses rotator interval + descends through intertubercular sulcus (bicipital groove)
- Insertion: radial tuberosity (conjoined distal tendon of the short and long head)
Tendon of Long Head of Biceps Brachii
- attached to anterosuperior aspect of glenoid rim with fibers to
- anterosuperior labrum (biceps-labral complex)
- posterosuperior labrum (biceps-labral complex)
- supraglenoid tubercle
- base of coracoid process
- exits joint through intertubercular groove
- secured to intertubercular groove by transverse lig.
- surrounded by slinglike band of CHL superiorly and superior GHL anteriorly
= most superficial capsular structure of rotator interval blending with fibers of subscapularis + supraspinatus tendons at their insertions forming roof of rotator interval with
- larger (lateral) band
Insertion: greater tuberosity + fibers of supraspinatus tendon - smaller (medial) band crosses over biceps tendon + forms anterior covering around biceps tendon blending with fibers of subscapularis tendon
Insertion: proximal aspect of lesser tuberosity
- Origin: lateral aspect of base of coracoid process
- Course: runs parallel to superior glenohumeral lig. posteriorly + laterally to fuse with joint capsule
Variations of insertion:
- into rotator interval
- to supraspinatus tendon / subscapularis tendon
- to supraspinatus + subscapularis tendons






= strong triangular fibrous band that extends from coracoid process to acromion forming protective arch superficial to rotator cuff
= triangular space between superior border of subscapularis tendon + anterior border of supraspinatus tendon
= portion of glenohumeral joint capsule that is not reinforced by overlying rotator cuff muscles
- Apex: combined fibers from subscapularis tendon with contributions from supraspinatus tendon and CHL + posterior lamina of tendon of pectoralis major muscle (“transverse ligament”) bridging bicipital groove
- Base: coracoid process with origin of coracohumeral lig. medially
- Content: intraarticular portion of long biceps tendon, coracohumeral ligaments
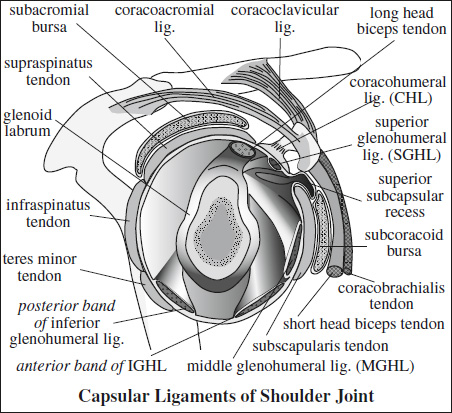
= thickened collagenous bands of joint capsule functioning as shoulder stabilizers
Superior Glenohumeral Ligament (SGHL)
= most consistently identified capsular ligament
- Function: passive restraint to inferior translation of adducted shoulder
- Origin: superior glenoid tubercle (= upper pole of glenoid cavity) just anterior to origin of biceps tendon and base of coracoid process
- Course: passes between supraspinatus + subscapularis in plane perpendicular to middle glenohumeral ligament + parallel to coracoid process
- Insertion: lesser tuberosity at bicipital groove
- merges with coracohumeral ligament in rotator cuff interval
- best visualized on transverse CT / MR
Middle Glenohumeral Ligament (MGHL)
= varies most in size + attachment; may be absent
- Function: limits anterior translation with external rotation + moderate abduction
- Origin: medially on scapular neck / superior portion of anterior glenoid rim
- Course: obliquely from superomedial to inferolateral
- Insertion: medial from lesser tuberosity at anterior aspect of anatomic neck
- taught during external rotation
- blends into capsular sheath of subscapularis tendon
- may be thick + cordlike
- best visualized on sagittal / transverse CT / MR
Inferior Glenohumeral Ligament (IGHL)
= important stabilizer of anterior shoulder joint
Function: resists anteroinferior glenohumeral translation
Course: from anteroinferior labrum to humeral metaphysis
- ligament + labrum function as single unit
= inferior glenohumeral labral-ligamentous complex(IGHLC) - taught during ABER position
- attaches to inferior ⅔ of the circumference of the entire labrum for a variable distance
- forms sleeve of continuous tissue with glenoid rim, capsule, periosteum, humeral metaphysis
- best visualized on MR arthrography / joint effusion
Parts:
- Anterior band of IGHL = thickened anterior-superior extent of ligament
- Critical to passive joint stabilization!
- Axillary pouch
- Posterior band of IGHL (usually thinner)
Normal Anatomic Variants of Shoulder
Sublabral Foramen = Sublabral Hole
= sublabral hole between labrum + glenoid
- Prevalence: 12% of individuals
- Location: 2 o'clock position anterior to biceps tendon attachment
- may coexist with sublabral recess
- DDx: labral tear (isolated tears are rare in this region)
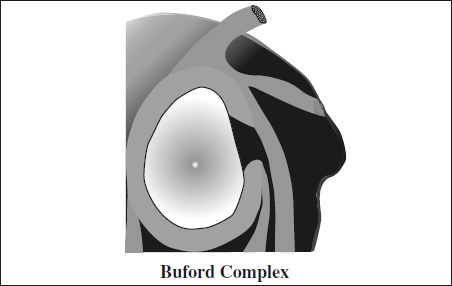
Buford Complex
= cordlike thickening of middle glenohumeral ligament directly attaching to anterosuperior glenoid + absence of anterosuperior labrum
- Prevalence: 1.5% of individuals
- Location: 2 o'clock position anterior to biceps tendon attachment
- course of middle glenohumeral ligament can be followed on serial images from origin to insertion
- may coexist with sublabral recess
- DDx: displaced anterosuperior labral fragment
Cysts and Bursae of Shoulder
- Subacromial-subdeltoid bursa
- Superior subscapular recess / subscapularis bursa
Location: between subscapularis muscle + anterior surface of scapula with extension above superior margin of subscapularis tendon- Foramen of Weitbrecht
= opening between SGHL and MGHL - Foramen of Rouvière
= opening between MGHL and IGHL
- Foramen of Weitbrecht
- Subcoracoid bursa
Location: between anterior surface of subscapularis muscle + coracoid process with extension along merged tendons of coracobrachialis m. + short head of biceps- no communication with glenohumeral joint
- ± communication with subacromial-subdeltoid bursa
- often associated with rotator cuff + interval tears
- AC joint cyst
- Glenoid labral cyst