- Linear fracture (most common type)
- deeply black sharply defined line
DDx:- Vascular groove, esp. temporal artery (gray line, slightly sclerotic margin, branching like a tree, typical location (temporal artery projects behind dorsum sellae)
- Suture
- deeply black sharply defined line
- Depressed fracture
- often palpable
- bone-on-bone density
Rx: surgery indicated if depression >3–5 mm ← arachnoid tear / brain injury
N.B.: CT / MR mandatory to assess extent of underlying brain injury - Skull-base fracture = basilar skull fracture
- rhinorrhea (CSF); otorrhea (CSF / hemotympanum)
- raccoon eyes = periorbital ecchymosis
- basic rules for skull fractures:
- overlying soft-tissue injury / hematoma
- sharp nonsclerotic border, often crossing sutures
- may bifurcate
- increase in diameter as fracture approaches suture
- diastasis of suture
- pneumocephalus
- air in sulci
- air-fluid level in sinuses
Cx: infection, acute / delayed cranial nerve deficit, vascular laceration / dissection / occlusion / infarction
DDx: suture (same diameter, interdigitating “zigzag” pattern)
- Healing skull fracture
- infants: in 3–6 months without a trace
- children (5–12 years): in 12 months
- adults: in 2–3 years
- persistent lucency mimicking vascular groove
Cx: leptomeningeal cyst (= growing fracture)

[René Le Fort (1869–1951), French surgeon]
◊All Le Fort fractures involve the pterygoid process!
- Le Fort I = transverse (horizontal) maxillary fracture caused by blow to premaxilla
Fracture line:- alveolar ridge
- lateral aperture of nose
- inferior wall of maxillary sinus
- detachment of alveolar process of maxilla
- teeth contained in detached fragment
- Le Fort II = “pyramidal fracture”
- May be unilateral
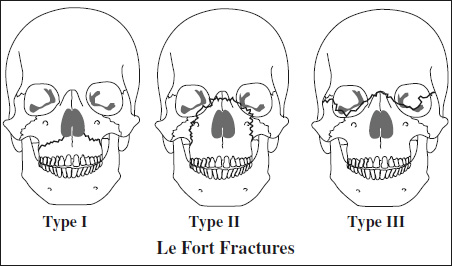
Fracture line: arch through- posterior alveolar ridge
- medial orbital rim
- across nasal bones
- separation of midportion of face
- floor of orbit + hard palate + nasal cavity involved
- Le Fort III = “craniofacial disjunction”
Fracture line: horizontal course through- nasofrontal suture
- maxillofrontal suture
- orbital wall
- zygomatic arch
- separation of entire face from base of skull
Prevalence: involved in 15% of skull-base fractures
- CSF rhinorrhea / otorrhea; hemotympanum
- “battle” sign = mastoid region ecchymosis
- raccoon eyes = periorbital ecchymosis; 7th / 8th nerve palsy
- muscular dysfunction: problems with ocular motility, mastication, speech, swallowing, eustachian tube function
- air-fluid level in sinuses + mastoid
- axial thin-slice high-resolution CT for best delineation of fractures
- water-soluble intrathecal contrast material for CSF fistula
Frequency: 14–22% of skull fractures
Mechanism: motor vehicle crash (45–47%), fall (31–33%), assault (11–12%)
Cause of conductive hearing loss of temporal bone fracture:
- Hemotympanum
- Disruption of tympanic membrane
- Disruption of the ossicular chain:
- commonly incus injury:
- incudostapedial joint subluxation
- malleoincudal subluxation
- incus dislocation
- dislocation of the malleoincudal complex
- less commonly: stapedial and mallear fracture
- commonly incus injury:
A common complication of temporal bone fractures is hearing loss, either sensorineural, conductive, or mixed.
Longitudinal Fracture of Temporal Bone (75%)
= fracture parallel to long axis of petrous pyramid typically traversing middle ear cavity with frequent disruption of ossicles → conductive hearing loss
Line of force:
- usually extralabyrinthine from lateral to medial terminating in foramen lacerum; commonly involving EAC (external auditory canal), tegmen tympani, squamosa of temporal bone
Subtypes:
- anterior to labyrinthine structures toward eustachian tube + middle cranial fossa (common)
Cx: epidural hematoma in middle cranial fossa ← vascular injury to middle meningeal artery - posterior to labyrinth, toward jugular foramen and posterior cranial fossa (less common)
Commonly associated with: fracture of temporal squamosa + parietal bone
- bleeding from EAC ← disruption of tympanic membrane
- otorrhea ← CSF leak with ruptured tympanic membrane (rare)
- conductive hearing loss ← dislocation of auditory ossicles (most commonly incus as the least anchored ossicle)
- NO neurosensory hearing loss
- facial nerve palsy (7–20%) ← edema / fracture of facial canal near first genu / anterior tympanic segment of facial nerve; frequent spontaneous recovery
- pneumocephalus
- herniation of temporal lobe
- incudostapedial joint dislocation (weakest joint):
- “ice cream” (malleus) has fallen off the “cone” (incus) on direct coronal CT scan
- fracture of “molar tooth” on direct sagittal CT scan
- mastoid air cells opaque / with air-fluid level
Plain film views: Stenvers / Owens projection
Cx: ossicular injury, tympanic membrane rupture, hemotympanum → conductive hearing loss, (rarely) facial n. injury
Transverse Fracture of Temporal Bone (25%)
= fracture perpendicular to long axis of petrous pyramid
Line of force:
- anterior to posterior originating in occipital bone (near jugular foramen / foramen magnum) extending anteriorly across the base of skull + across the petrous pyramid into middle cranial fossa; commonly passing through / near vestibular aqueduct with variable involvement of otic capsule
Subtypes:
- medial relative to arcuate eminence
Course: traversing fundus of IAC- ± complete SNHL ← transection of cochlear n.
- lateral relative to arcuate eminence
Course: traversing bony labyrinth
Associated with: ± perilymphatic fistula ← injury of stapes footplate- ± complete SNHL
- irreversible sensorineural hearing loss ← fracture line across apex of IAC / labyrinthine capsule with injury to both parts of cranial nerve VIII)
- persistent vertigo (benign paroxysmal positional vertigo resolves in 6–12 months, perilymphatic fistula, cupulolithiasis = otolith detachment, trauma to semicircular canals)
- facial (cranial nerve VII) nerve palsy in 50% (injury in IAC); less frequent spontaneous recovery because of disruption of nerve fibers
Site: labyrinthine segment, geniculate ganglion - rhinorrhea ← CSF leak with intact tympanic membrane
- bleeding into middle ear
Plain film views: posteroanterior (transorbital) + Towne projection
Mixed Temporal Bone Fracture
Temporal bone fractures may be complex with mixed features of both longitudinal + transverse fractures.
= combination of longitudinal + transverse fractures
- sensorineural hearing loss ← disruption of otic capsule
- conductive hearing loss ← ossicular injury
- Quite common!
Ossicular Injury
- persistent conductive hearing deficit after healing of tympanic membrane / resorption of middle ear debris
- Ossicular dislocation: incudostapedial separation >complete separation of incus including incudomalleolar separation >dislocation of malleoincudal complex >stapediovestibular dislocation
- Ossicular fracture: long process of incus >crura of stapes >neck of malleus
= “TRIPOD” FRACTURE = MALAR / ZYGOMATIC COMPLEX FRACTURE
Cause: direct blow to malar eminence
- loss of sensibility of face below orbit
- deficient mastication
- double vision / ophthalmoplegia
- facial deformity
Fracture line:
- lateral wall of maxillary sinus
- orbital rim close to infraorbital foramen
- floor of orbit
- zygomaticofrontal suture / zygomatic arch
= isolated fracture of orbital floor
Cause: sudden direct blow to globe (ball or fist) with increase in intraorbital pressure transmitted to weak orbital floor
- diplopia on upward gaze (entrapment of inferior rectus + inferior oblique muscles)
- enophthalmos
- facial anesthesia
Associated with: fracture of the thin lamina papyracea (= medial orbital wall) in 20–50%
- soft-tissue mass extending into maxillary sinus ← herniation of orbital fat
- complete opacification of maxillary sinus ← edema + hemorrhage
- depression of orbital floor (= orbital process of maxilla)
- posttraumatic atrophy of orbital fat → enophthalmos
- opacification of adjacent ethmoid air cells
- disruption of lacrimal duct
Anderson & Montesano Types (I–III):
- I = stable comminution-impaction with minimal / no fracture displacement ← axial loading injury
- II = linear skull base fracture extending into occipital condyle ← direct blow to head
- III = unstable avulsion fracture (75%) of occipital condyle ← avulsion injury of alar ligaments ← forced rotation + lateral bending
Tuli Types (1, 2A, 2B)
- 1 = nondisplaced fracture
- 2A = displaced fracture WITHOUT ligamentous instability
Rx: rigid collar - 2B = displaced fractures WITH ligamentous instability
Rx: surgical intervention