◊Clearing of the cervical spine on clinical grounds has become the standard of care in alert adult patients.
Factors associated with higher risk of fracture:
- Glasgow Coma Score <14
- Neck tenderness
- Loss of consciousness
- Neurologic deficit
- Drug ingestion
- Specific mechanism of injury: motor vehicle accident, fall from a height >3 m
Indications for screening CT of cervical spine:
- high-risk adult patients (= >5% pretest probability of injury) defined by:
- High-speed (>35 mph) motor vehicle accident
- Crash resulting in death at scene of accident
- Fall from height >3 m (10 feet)
- Significant closed head injury (intracranial hemorrhage seen on CT)
- Neurologic signs / symptoms referred to C-spine
- Pelvic / multiple extremity fractures
Frequency: 1–3% of all trauma cases;
C2, C6 >C5, C7 >C3, C4 >C1
◊Cervical spine trauma accounts for ⅔ of all spinal cord injuries!
- neurologic / spinal cord damage (39–50%)
Location:
- upper cervical spine = C1/2 (19–25%): atlas (4%), odontoid (6%)
- lower cervical spine = C3–7 (75–81%)
- cervicothoracic junction (9–18%)
- multiple noncontiguous spine fractures (15–20%)
Site: vertebral arch (50%), vertebral body (30%), intervertebral disk (25%), posterior ligaments (16%), dens (14%), locked facets (12%), anterior ligament (2%)
Associated with injury to:
- head (70%), thoracic spine (15%), lumbar spine (10%), thorax (35%), pelvis (15%), upper extremity (10%), lower extremity (30%)
N.B.: 5–8% of patients with fractures may have normal radiographs!
- Most missed fractures involve C2 (34%), C6-7 (14%), C4 (12%), C1 (8%), occipital condyles
- C7–T1 space not visualized in at least 26% of all trauma patients
Normal range of motion: 10–20° during flexion and extension; 4–12° of lateral tilting
Cx: neurologic deterioration with delay in diagnosis
- HYPERFLEXION INJURY (46–79%)
- Odontoid fracture
- Simple wedge fracture (stable)
- Flexion teardrop fracture = avulsion of anteroinferior corner by anterior ligament (unstable)
- Most severe + unstable injury of C-spine
Location: C5, C6, C7- triangular fragment in soft tissues anterior to vertebral body
- retrolisthesis
- widening of facets
- narrowing of spinal canal
- mild kyphosis
Associated with: ligamentous tears, spinal cord compression
Subaxial Injury Classification and Scoring (CT Severity Score for Entire Spine, 2007)*
Injury Category Point Value Injury Morphology Compression 1 Burst 2 Distraction 3 Translation / rotation 4 Discoligamentous complex Intact 0 Indeterminate 2 Disrupted 3 Neurologic status Intact 0 Root injury 1 Spinal cord injury incomplete 2 complete 3 Cord injury + ongoing compression 4 Total Score:≤3 manageable without surgery
4 indeterminate;
≥5 need for surgical intervention* a separate score is given to each injured level
◊Triangular teardrop fracture without posterior element distraction / vertebral body translation should be characterized as (1) compression or (2) burst injury. - Anterior subluxation
- Bilateral facet lock = interlocking of articular surfaces (unstable)
- anterolisthesis of affected vertebra by ½ vertebral body width
- mild focal kyphosis
- soft-tissue swelling
- no rotation
- Anterior disk space narrowing
- Spinous process fracture = clay shoveler's fracture
= sudden load on flexed spine with avulsion fracture of C6 / C7 / T1 (stable) - Flexion instability = isolated rupture of posterior ligaments
- Dx may be missed without delayed flexion views
- no fracture
- interspinous widening
- loss of facet parallelism
- widening of posterior portion of disk
- anterolisthesis >3 mm
- focal kyphosis
- HYPEREXTENSION INJURY (20–38%)
Mechanism: impact on forehead / face, whiplash- High risk for neurologic deficit!
- Radiographs may be completely normal!
- Hyperextension dislocation
followed by immediate realignment- upper extremity paresthesia to complete quadriplegia
- disruption of anterior longitudinal ligament, annulus, intervertebral disk, lig. flavum
- prevertebral swelling ← hemorrhage + edema
- stripping of posterior longitudinal ligament
- tears of paraspinal muscles
- widening of disk space anteriorly
- avulsion of anteroinferior endplate
- transverse dimension of anteroinferior avulsion fragment greater than vertical dimension
- Extension teardrop fracture
= avulsion of intact fibers of anterior longitudinal ligament off anteroinferior endplate
Location: C2, C3- acute central cord syndrome (in up to 80%)
- vertical dimension of triangular fragment greater than transverse dimension
- Neural arch fracture of C1 (stable fracture = anterior ring + transverse ligament intact)
- vertically oriented fracture of posterior arch (stable if isolated / part of Jefferson burst fracture)
- Anterior arch fracture of C1
- biomechanically stable
- transverse fracture through inferior pole / midportion at attachment of atlantodental lig. / longus colli m.
- Uni- / bilateral laminar fracture commonly part of a burst fracture / pedicolaminar fracture-separation / flexion teardrop fracture
- extension into adjacent spinous process (frequent)
- Subluxation (anterior / posterior)
- Hangman's fracture
- FLEXION-ROTATION INJURY (12%)
- Unilateral facet lock (oblique views!, stable fracture)
- anterolisthesis <¼ vertebral body width
- “bow-tie” sign = the 4 rotated facets on LAT view
- decrease in spinolaminar space
- rotation of spinous process (on AP view)
- “naked facet” (on CT)
- Unilateral facet lock (oblique views!, stable fracture)
- VERTICAL COMPRESSION (4%)
= axial loading- Jefferson fracture
- Burst fracture = intervertebral disk driven into vertebral body below (fracture may be stable / unstable)
- loss of posterior vertebral body height with several fragments:
- sagittal fracture component extending to inferior endplate
- retropulsed fragment from posterior superior margin in spinal canal
- interpedicular widening
- posterior element fracture
Associated with: widening of apophyseal joints, fracture of posterior vertebral arches - loss of posterior vertebral body height with several fragments:
- LATERAL FLEXION / SHEARING (4–6%)
- Uncinate fracture
- Isolated pillar fracture
- Transverse process fracture
- Lateral vertebral compression
Normal Variants as Pitfalls in Cervical Trauma
- Congenital absence of posterior arch(es)
- Congenital cleft (smooth well-corticated)
- Os odontoideum
- Os terminale
- Partial ossification of atlanto-occipital membrane
- Ponticulus posticus = bone excrescence partially covering horizontally oriented vertebral artery
- Arcuate foramen = bone excrescence completely surrounding vertebral artery
Signs of Significant Cervical Vertebral Trauma
- most reliable + specific:
- widening of interspinous space (43%)
- widening of facet joint (39%)
- displacement of prevertebral fat stripe (18%)
- reliable but nonspecific:
- wide retropharyngeal space >7 mm (31%)
DDx: mediastinal hemorrhage of other cause, crying in children, S/P difficult intubation) - nonspecific:
- loss of lordosis (63%)
- anterolisthesis / retrolisthesis (36%)
- kyphotic angulation (21%)
- tracheal deviation (13%)
- disk space: narrow (24%), wide (8%)
Prevalence: 4% of cervical spine injuries, 25% of craniocervical injuries
Associated with: axis fracture (44%), fractures of C7 (25%), C2 pedicle (15%), extraspinal fractures (58%)
N.B.: A ring tends to fracture in more than one place!
Types:
- I Isolated fracture of posterior arch ← hyperextension
- II Isolated fracture of anterior arch (rare)
- III Bilateral posterior arch fractures + uni- / bilateral anterior arch fracture ← axial loading
- Jefferson fracture
[Sir Geoffrey Jefferson (1886–1961), neurosurgeon in Manchester, England]- comminuted burst fracture of ring of C1 (unstable) with 4 uni- / bilateral ipsilateral anterior + posterior fractures
- lateral displacement of lateral masses (self-decompressing) on AP view
DDx:Pseudo-Jefferson fracture = lateral offset of lateral masses of atlas without fracture = fusion anomaly of anterior / posterior arches of C1 (in children as lateral masses of atlas ossify earlier than C2)
- Jefferson fracture
- IV fracture of lateral mass ← excessive lateral flexion
- V Transversely oriented anterior arch fracture ← avulsion of longus colli / atlantoaxial ligament
Burst and lateral mass fractures are unstable and can be associated with tears of the transverse ligament, which may compromise the atlantodental relationship → dorsal displace-ment of dens → compression of thecal sac and its contents.
Prevalence: 17–20% of cervical spine fractures
Associated with: fractures of C1 in 8%
Odontoid / Dens Fracture (59%)
Prevalence: 59% of C2 fractures
- Type I avulsion fracture through odontoid tip (1–8%) at attachment of alar ligaments
- obliquely oriented fracture through tip of odontoid that is difficult to detect
Prognosis: bone fusion in almost 100% with collar / halo immobilization
- obliquely oriented fracture through tip of odontoid that is difficult to detect
- Type II fracture through base of dens (54–60%)
Cx: nonunion (in 26% of nonsurgical treatment, with fracture gap ≥6-mm increased to 67%)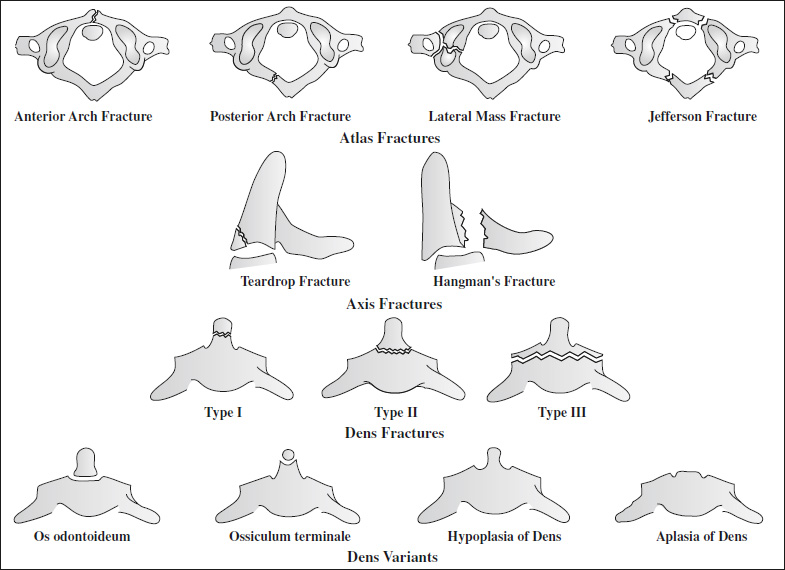
◊Axial CT alone misses >50%! - Type III horizontal subdental fracture (39–42%) through cancellous portion of body
Prognosis: heals in 88% with immobilization
DDx: os odontoideum, ossiculum terminale, hypoplasia of dens, aplasia of dens
Hangman's Fracture (23%)
= TRAUMATIC SPONDYLOLISTHESIS
Prevalence: 23% of C2 fractures, 4% of cervical fractures
- 2nd most common C2 fracture; unstable
Mechanism: direct impact to face ← compressive hyperextension / distractive hyperflexion
Associated with: neurologic sequelae in only 26%, atlas fracture in 6–26%, other cervical fractures in 8–32%
Types:
- I minimally displaced with <2-mm translation, NO angulation / posterior intervertebral disk space widening (stable)
- II anterior angulation >11° + anterior translation ← distractive flexion / compressive hyperextension
- III (7–10% of hangman fractures) ← severe distractive flexion + bilateral facet dislocation / fracture-dislocation
- bilateral vertical pars interarticularis fracture of C2 → separation of body from posterior arch → decompression of spinal canal
- fracture through posterior body of C2
- prevertebral soft-tissue swelling >5 mm at anterior-inferior margin of C2
- ± widening of C2-C3 disk space
- ± bilateral interfacetal dislocation
- anterior subluxation of C2 on C3:
- disruption of C1–C2 spinolaminar line
- disruption of C2–C3 posterior vertebral body line
- avulsion of anteroinferior corner of C2 (= rupture of anterior longitudinal ligament) = teardrop fracture