Differential Diagnosis of Nervous System Disorders
= shift of normal brain from high to low pressure through rigid structures of skull ←⇑ intracranial pressure
Cause: mass effect by primary / metastatic tumor, trauma, infection (abscess) / inflammation, intracranial hemorrhage, subdural hematoma, ischemia / infarction, acute hydrocephalus, iatrogenic (after lumbar puncture / pneumocephalus following craniotomy)
Classification:
- SUPRATENTORIAL HERNIATION
- Uncal (transtentorial)
- Central
- Cingulate (subfalcine)
- Transcalvarial
- Tectal (posterior)
- INFRATENTORIAL HERNIATION
- Upward (upward cerebellar / upward transtentorial)
- Tonsillar (downward cerebellar)
Subfalcine / Cingulate Herniation (most common)
= contralateral shift of midline structures under falx cerebri
= herniation of cingulate gyrus across falx cerebri
Risk: compression of one of anterior cerebral arteries
May be associated with: transtentorial herniation
- weakness / paresis of contralateral leg ← compression of parafalcine cortex
- weakness ± sensory changes of contralateral leg ← infarction of paracentral lobule / superior frontal gyrus ← compression of ACA / pericallosal artery
- somnolence ← raised intracranial pressure
- early signs:
- falx
- shift of ipsilateral cingulate gyrus beneath falx
- deviation of anterior falx with widened CSF space at contralateral side
N.B.: posterior falx remains relatively undisplaced due to greater height + rigidity - cingulate gyrus
- compression of contralateral cingulate gyrus
- corpus callosum
- depression of ipsilateral corpus callosum
- depression / elevation of contralateral corpus callosum
- ventricle
- compression / effacement of ipsilateral ventricle with amputation of ipsilateral frontal horn
- falx
- late signs:
- displacement of lateral ventricle to opposite side
- obstruction of foramen of Monro → contralateral dilatation of the lateral ventricle + subependymal edema
- infarction of cingulate gyrus
- compression of anterior cerebral artery → infarction of ACA territory
Assessment: degree of greatest displacement of septum pellucidum / falx measured in mm relative to a straight line drawn through anterior and posterior falcine attachments on axial image
Prognosis: good with shift of <5 mm; poor with shift >15 mm
Cx: traumatic aneurysm of ACA / pericallosal artery
Transtentorial (Central) Herniation
= herniation of brain up / down across tentorium cerebelli
Tentorium cerebelli = inelastic reflection of dura
Connected to: occipital bone posteriorly, petrous temporal bone laterally, clinoid processes anteriorly
Content: transverse sinus, straight sinus
Tentorial hiatus / incisura
Content: cerebral peduncles + brainstem
Alert: NO lumbar puncture with effacement of basal cisterns + displacement of 4th ventricle!
Descending Transtentorial Herniation
= downward herniation of brain toward posterior fossa
- oculomotor nerve (cranial n. III) palsy:
- ipsilateral dilated pupil (= mydriasis) due to uncal herniation → compression of parasympathetic fibers traveling on outside of CN III → unopposed sympathetic activity to iris sphincter m.
- abnormal extraocular muscle function (except for superior oblique m., lateral rectus m., levator palpebrae superioris m.)
- ipsilateral hemiparesis (on side of expanding lesion) (false localizing sign = Kernohan notch syndrome) due to severe lateral translation of midbrain against opposite tentorial edge → compression of opposite corticospinal tracts above decussation
- permanent anterograde amnesia ← infarction of uncal / parahippocampal gyrus ← arterial compression
- permanent visual field defect ← temporal / occipital lobe infarction ← compression of calcarine branch of PCA against tentorium
Location and degree of herniation:
- anterior / uncal herniation (see below)
- posterior: herniation of parahippocampal gyrus
- total: herniation of entire hippocampus
- compression of ipsilateral cerebral peduncle
- compression of contralateral cerebral peduncle → notching of midbrain (= Kernohan notch)
- compression of aqueduct of Sylvius → early dilatation of temporal horn → obstructive hydrocephalus
- widening of contralateral temporal horn
- widening (obliteration) of ipsilateral (contralateral) basilar (ambient + quadrigeminal) cisterns
Cx:
- Occipital infarction ← compression of ipsilateral posterior cerebral artery against cerebral peduncle by uncus + parahippocampal gyrus
- effacement / displacement of ipsilateral PCA
- Duret hemorrhage = hemorrhage in median / paramedian mesencephalon / tectum ← stretching of pontine perforators ← downward displacement of pons
- Respiratory arrest
Uncal / Anterior Transtentorial Herniation
= herniation of uncus (most medial part of temporal lobe) across tentorium cerebelli into suprasellar cistern
◊Most common subtype of transtentorial herniation caused by lesions in anterior half of brain
- uncus displaced into suprasellar cistern → pressure on midbrain + brainstem
- truncation of six-pointed star appearance of suprasellar cistern
Risk: (1) compression of midbrain (brainstem)
(3) Kernohan notch syndrome
Ascending Transtentorial / Cerebellar Herniation
= displacement of cerebellum through tentorial incisura superiorly = upward (superior vermian) displacement
Cause: slowly growing cerebellar / brainstem process, infarction
- nausea & vomiting → obtundation → coma
- compression + anterior displacement of 4th ventricle
- occlusion of aqueduct → obstructive hydrocephalus
- narrowing / effacement of ambient + quadrigeminal cistern
- compression of pons against clivus
- upward displacement of cerebellar vermis
- superior displacement of tectum
- “spinning top” appearance of midbrain due to bilateral compression on posterolateral aspect of midbrain
- downward displacement of cerebellar tonsils
Cx:
- basilar artery compression ← displacement of midbrain / pons against clivus
- compression of vein of Galen / basal vein of Rosenthal → parenchymal congestion
- compression of posterior cerebral + superior cerebellar arteries ← superior displacement of cerebellum
Alar / Transalar / Retroalar / Sphenoid Herniation
= herniation of frontal lobe posteriorly across edge of sphenoid ridge
Associated with: transtentorial + subfalcine herniation
- paucity of clinical symptomatology, clinically occult
- posterior / descending: frontal lobe mass
- frontal lobe displaced posteriorly
- posterior displacement of sylvian fissure, temporal lobe + horizontal segment of MCA
- anterior / ascending: temporal lobe / insula lesion
- temporal lobe displaced anteriorly
Transforaminal / Tonsillar Herniation
= herniation of inferior mesial portions of cerebellum (= inferior tonsils) downward through foramen magnum
Commonly associated with: ascending (⅔) or descending (⅓) transtentorial herniation
- neck pain, nystagmus, vomiting (in conscious patient)
- Cushing response (= irregular respiration, bradycardia, hypertension) as warning sign in unconscious patient
- decerebrate posturing
Risk: compression of medulla → respiratory arrest → cardiovascular collapse → coma → death
- cerebellar tonsils at level of dens on axial images
- cerebellar tonsils ≥5 mm below foramen magnum (= line connecting basion with opisthion) in adults; ≥7 mm in children on sagittal / coronal images
- effacement of 4th ventricle / aqueduct → hydrocephalus of 3rd + lateral ventricles with transependymal CSF flow
- ± concurrent upward displacement of vermis
Cx: compression of vulnerable PICA → cerebellar infarction
Alert: Known complication of lumbar puncture performed in context of elevated intracranial pressure!
Transcalvarial / External Herniation
= brain protrusion through fracture / surgical site of skull
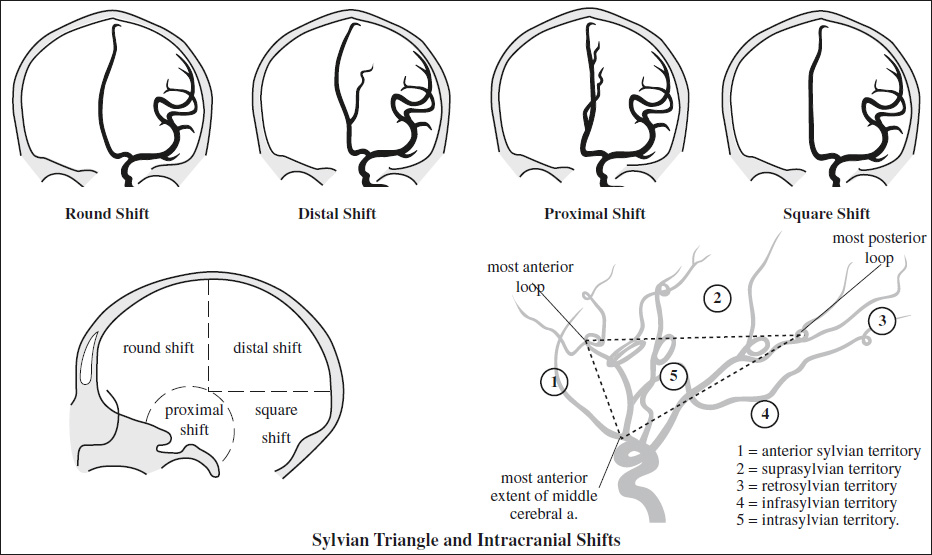
- ARTERIAL SHIFT
- Pericallosal arteries
- Round shift = frontal lesion anterior to coronal suture
- Square shift = lesion behind foramen of Monro in lower half of hemisphere
- Distal shift = posterior to coronal suture in upper half of hemisphere
- Proximal shift = basifrontal lesion / anterior middle cranial fossa including anterior temporal lobe
- Sylvian triangle
= branches of MCA within sylvian fissure on outer surface of insula form a loop upon reaching the upper margin of the insula; serves as angiographic landmark for localizing supratentorial masses
Location of lesion:- anterior sylvian frontal region
- suprasylvian posterior frontal + parietal
- retrosylvian occipital, parietooccipital
- infrasylvian temporal lobe + extracerebral region
- intrasylvian usually due to meningioma
- lateral sylvian frontal, frontotemporal, parietotemporal
- central sylvian deep posterior frontal, basal ganglia
- Pericallosal arteries
- CEREBRAL VEINS
= indicate the midline of the posterior part of the forebrain showing the exact location of the roof of the 3rd ventricle