= presence of ≥1 lateral curves of the vertebral column in the coronal plane with a Cobb angle of ≥10°
◊A curve of <10° represents spinal asymmetry and NOT scoliosis, is asymptomatic and nonprogressive!
Mechanism: rotation of vertebrae in axial plane → discrepant axial loading between ventral + dorsal portions
Etiology:
- PRIMARY = idiopathic (80%)
- Infantile (0–3 yrs.): M÷F=3.5÷1; levoscoliosis; self-limited
- Juvenile (4–10 yrs.): progression in 70–95%
- Adolescent (11–18 yrs.): M÷F=1÷4; dextroscoliosis; progression in 5%
- SECONDARY
- congenital (10%) with progression in 75%
- Osteogenic: wedge-shaped vertebra, hemivertebra, fused vertebra, unilateral bar
- Neuropathic: tethered cord, syringomyelia, Chiari malformation, (myelo)meningocele, diastematomyelia
- developmental
- Skeletal dysplasia: achondroplasia
- Skeletal dysostosis: neurofibromatosis, osteogenesis imperfecta
- Degenerative scoliosis
- Traumatic scoliosis
- neuromuscular
- Neuropathic (acquired): cerebral palsy, spinocerebellar degeneration, poliomyelitis
- Myopathic: muscular dystrophy
- tumor-associated
- Osseous: osteoid osteoma, osteoblastoma
- Extraosseous: extramedullary (eg, neurofibroma) / intramedullary (eg, astrocytoma) tumor
- congenital (10%) with progression in 75%
A focal short-segment scoliosis or painful scoliosis should raise suspicion for an underlying lesion.
Nomenclature:
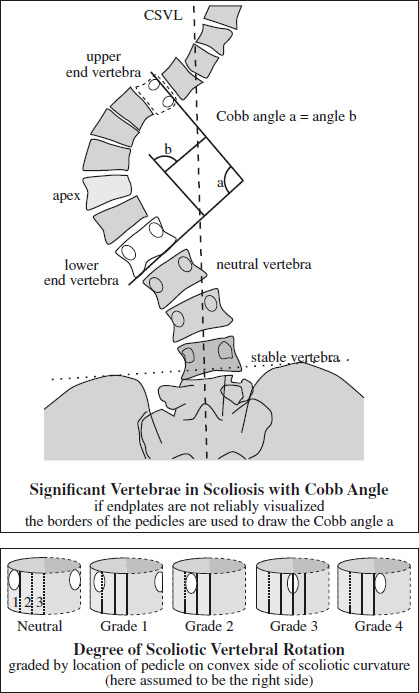
- apex = vertebra / disk with the greatest rotation / farthest deviation from center of vertebral column
- end vertebra = vertebra with maximum tilt toward apex of curvature; used to measure Cobb angle
- neutral vertebra = vertebra without rotation (= symmetric pedicles) on standing frontal radiograph
- stable vertebra = vertebra farthest cephalad roughly bisected by CSVL below end vertebra of distal curve
- CSVL = central sacral vertical line = line drawn perpendicular to tangential line across iliac crests bisecting sacrum
- Primary and Secondary Curves
- Major curve = primary structural curve with a Cobb angle of >25° on ipsilateral bending; largest abnormal curve that develops first; not correctable with ipsilateral bending
- Minor curve = secondary nonstructural compensatory smaller curve that develops later by repositioning the head and trunk over pelvis to maintain balance; correctable with ipsilateral bending
- Major curve = primary structural curve with a Cobb angle of >25° on ipsilateral bending; largest abnormal curve that develops first; not correctable with ipsilateral bending
- Vertebral Balance
- Plumb line = vertical line drawn downward from center of C7 parallel to lateral edge of radiograph
- Coronal imbalance = distance between CSVL + plumb line >2 cm on frontal x-ray; plumb line to right (left) of CSVL = positive (negative) imbalance
- Sagittal imbalance = distance between posterosuperior aspect of S1 + plumb line >2 cm on lateral x-ray; plumb line anterior (posterior) to S1 = positive (negative) imbalance
- Vertebral Rotation (Nash-Moe method)
Cobb angle: angle formed by intersection of 2 lines parallel to endplates of superior + inferior end vertebrae or intersection of the 2 lines drawn perpendicular to the endplate lines
- Accuracy: ± 5°
- Progressive curve: angle increase of ≥5°
- Limitation: 2-D radiograph describing a 3D deformity with vertebral rotation
- Pitfalls: diurnal variation of 5° (worse in afternoon); 2–7° measurement error; 5–10° interobserver error; actual angle may be 20% greater than plotted depending on accuracy + reproducibility of patient positioning on frontal x-ray
Progression: parallels spinal growth; after skeletal maturity at <30° no progression, at 30–50° increase by 10–15° per year, at 50–75° increase by 1° per year
Prognosis: with Cobb angle >50° higher rate of back pain + mortality associated with cardiopulmonary Cx