= break in the interarticular portion of a vertebra
pars interarticularis = junction of vertebral pedicle, lamina, superior + inferior articular facets
Pars interarticularis abnormalities are a spectrum of nonunion, spondylolysis and stress without spondylolysis.
Prevalence: 3–7% of population; in 30–70% other family members afflicted
Age: early childhood; M÷F = 3÷1; Whites÷Blacks = 3÷1
Cause:
- Chronic low-grade trauma: stress (fatigue) fracture of pars interarticularis from repetitive minor trauma (in most); during teenage growth spurt; common in gymnastics (30%), ballet, scrubbing floors, lifting heavy objects, diving, contact sports (college football player (20%), wrestler (28%), soccer, hockey, lacrosse)
- Developmental deficiency:
- hereditary hypoplasia of pars → insufficiency fracture; eg, pars defect in 34% of Eskimos
- congenital malformation: frequently associated with spina bifida occulta of S1, dorsally wedge-shaped body of L5, hypoplasia of L5; HOWEVER: no pars defects have been identified in fetal cadavers
- Secondary spondylolysis: neoplasm, osteomyelitis, Paget disease, osteomalacia, osteogenesis imperfecta
- activity-related low back pain + hamstring tightness in 50% (if associated with degenerative disk disease / spondylolisthesis)
Location: L5 (67–95%); L4 (15–30%); L3 (1–2%); in 75% bilateral
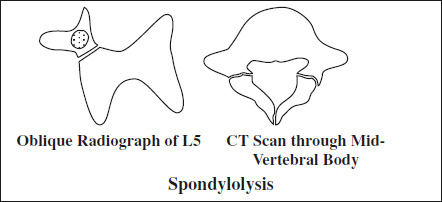
Plain film (57% PPV):
- radiolucent band ± sclerotic margin resembling the collar of a “Scottish dog” (on oblique view)
- may be associated with spondylolisthesis
- subluxation of involved vertebra (if pars defect bilateral)
- Wilkinson syndrome = reactive sclerosis + bony hypertrophy of contralateral pedicle + lamina ← stress changes related to weakening of neural arch in unilateral pars defect
CT:
- pars defect located 10–15 mm above disk space
- inner contour of spinal canal interrupted
NUC bone scintigraphy:
Sensitivity: SPECT/CT >SPECT >planar imaging
Spectrum: uni- / bilateral stress or break
- stress (50%) = uni- / bilateral focal radiotracer uptake of pars interarticularis WITHOUT break BUT osteosclerosis
- active spondylysis = uni- / bilateral focal radiotracer uptake + osteolysis (CLASSIC)
- nonunion (pseudarthrosis) = NO radiotracer uptake + break in pars interarticularis and sclerosis along margins of defect
Cx:
- Spondylolisthesis (uncommon; most likely before 16 years of age)
- Vertebral pedicle fracture (rare; typically unilateral fracture with contralateral spondylolysis; best seen on SAG reformatted CT)
Spondylolysis of Cervical Spine
= progressive degeneration of intervertebral disks leading to proliferative changes of bone + meninges; more common than disk herniation as a cause for cervical radiculopathy
Prevalence: 5–10% at age 20–30; >50% at age 45; >90% by age 60
- spastic gait disorder
- neck pain
Location: C4-5, C5-6, C6-7 (greater normal cervical motion at these levels)
Sequelae:
- direct compression of spinal cord
- neural foraminal stenosis
- ischemia due to vascular compromise
- repeated trauma from normal flexion / extension
DDx of myelopathy:
- rheumatoid arthritis, congenital anomalies of craniocervical junction, intradural extramedullary tumor, spine metastases, cervical spinal cord tumor, arteriovenous malformation, amyotrophic lateral sclerosis, multiple sclerosis, neurosyphilis