Bone and Soft-Tissue Disorders
Cause: acute injury; degeneration related to aging; tear contributes to degenerative joint disease
Prevalence: increases with age
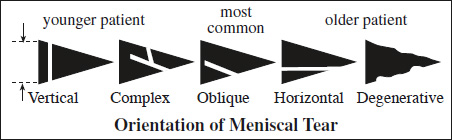
Type of cross-sectional tear pattern:
- vertical tear with longitudinal / radial / oblique surface pattern
- horizontal tear with longitudinal / oblique / cleavage surface pattern
- mixed pattern
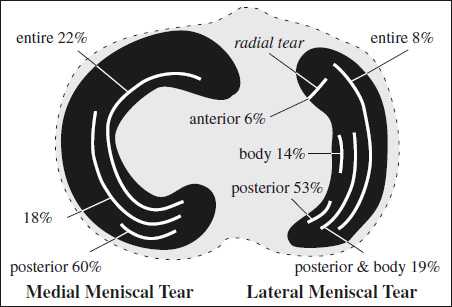
Site of injury:
- medial meniscus (MM) in 45%:
- no isolated tears of body
- isolated tear of anterior horn in 2%
- lateral meniscus (LM) in 22%:
- tear of posterior horn in 80% of all LM tears
- more common in acute injury of young individuals
- with ACL tear → increased prevalence of peripheral tears → decreased sensitivity for tear detection in LM
- isolated tear of anterior horn in 16%
- both menisci involved in 33%
- posterior horn of both menisci: constrained MM >LM
Associated with: ligamentous injury
- asymptomatic in up to 20% of older individuals
MR:
- DIRECT SIGNS (in the absence of prior surgery):
- increased signal extending to articular surface:
- “two-slice-touch” rule = ≥2 images with signals contacting the surface (94% PPV in MM, 96% PPV in LM)
- 1 image with signal contacting surface (43% PPV in MM, 18% PPV in LM) reported as possible tear
- Diagnosis of tear hinges on surface involvement!
- Truncation artifact + magic angle artifact may cause increased intrameniscal signal!
- distortion of meniscal shape
- increased signal extending to articular surface:
- INDIRECT SIGNS
- meniscal cyst (meniscal tear in 98–100%)
= synovial fluid accumulation in degenerated tissue
Location: intrameniscal, meniscocapsular margin, parameniscal- cyst in continuity with horizontal cleavage / complex meniscal tear
- meniscal extrusion
= peripheral margin of meniscus extends ≥3 mm beyond edge of tibial plateau
N.B.: Exclude hypertrophic osteophyte for determination of outer margin!
Pathophysiology: disruption of circumferentially oriented collagen bundles → loss of meniscal hoop strength
Cause: root tear, complex tear, large radial tear, severe meniscal degeneration- 76% of medial root tears have extrusion
- 39% of extrusions have medial root tears
- subchondral bone marrow edema
= superficial edema adjacent to meniscal attachment site paralleling articular surface <5 mm deep- medial meniscus (in 60%): 64–70% sensitive, 94–100% specific
- posterior lip medial tibial plateau bone bruise (64% PPV for tear in posterior horn of MM)
- lateral meniscus (in 90%): 88–89% sensitive, 98–100% specific
- medial meniscus (in 60%): 64–70% sensitive, 94–100% specific
- torn popliteomeniscal fascicle (79% PPV)
- meniscal cyst (meniscal tear in 98–100%)
MR sensitivity, specificity, and accuracy:
|
- MR has a high negative predictive value!
- 60–97% accuracy for arthrography
- 84–99% accuracy for arthroscopy (poor at posterior horn of medial meniscus)
Interpretative / Diagnostic Error
(12% for experienced radiologist)
- anatomic error
- FN: tear mistaken for normal anatomic structure
- FP: normal anatomic structure mistaken for a tear
- technique-related error obscuring a tear
- Arterial pulsation
- Healed tear = retained abnormal increased SI
- Magic-angle effect = collagen fibers oriented at 55° relative to magnetic field
- often seen in upslope medial segment of LM posterior horn
Lateral meniscus: 5.0% FN (middle + posterior horn)
1.5% FP (posterior horn)
Medial meniscus: 2.5% FN (posterior horn)
2.5% FP (posterior horn)
Pitfalls in Diagnosing Meniscal Tears
- Normal variants simulating tears
- Superior recess on posterior horn of MM
- Popliteal hiatus
- Transverse ligament
- Meniscofemoral ligaments
- Oblique meniscomeniscal ligament (1–4%)
- Soft tissue between capsule + medial meniscus
- Diskoid meniscus
- Healed meniscus
- persistent grade 3 signal at least up to 6 months
- S/P meniscectomy (false-positive type IV finding)
- Globular / linear increase in SI (grade 1 /2 signal)
Cause:- internal mucinous degeneration in adults
- normal vascularity in children + young adults
- acute contusion in trauma
- Tears difficult to detect on SAG images ← volume averaging
- better depiction on COR images for
- Small radial tear
- Horizontal tear of body
- Bucket-handle tear
- AXIAL images helpful for detection of
- Small radial tear
- Displaced tear
- Peripheral tear of posterior horn of LM
- better depiction on COR images for
Easily Missed Meniscal Injury
- Radial tears
- Displaced flap tears
- Meniscocapsular separation
= CLEAVAGE TEAR
= tear oriented parallel to tibial plateau
- involving either articular surface / central free edge
- dividing meniscus into superior + inferior halves
Cause: degenerative in patients >40 years
Associated with: parameniscal cyst formation ← direct communication with joint fluid
- horizontally oriented line of high signal intensity contacting meniscal surface / free edge
Rx: débridement of smaller unstable meniscal leaf + decompression of associated parameniscal cyst
= tear oriented parallel to long axis / outer margin of meniscus + perpendicular to tibial plateau dividing meniscus into central + peripheral halves
Cause: significant knee trauma in younger patient
MR Classification of Meniscal Signal Intensity vs. Injury
|
Site: propensity to involve peripheral ⅓ of meniscus + posterior horn (difficult diagnosis for LM because of complex attachment anatomy)
- vertically oriented line of high SI contacting one / both articular surfaces (full / partial-thickness tear)
- NO involvement of free edge of meniscus
- disruption of posterosuperior popliteomeniscal fascicle = high PPV for tear of LM posterior horn
Close association with: ACL tear (in 90% for MM, in 83% for LM)
Rx: may be amenable to repair if
- in vascularized (peripheral) outer 3–5 mm
- between 7 and 40 mm long
= TRANSVERSE TEAR
= tear perpendicular to tibial plateau + long axis / free edge of meniscus → disruption of meniscal hoop strength → dramatic loss of function + possible meniscal extrusion
- tears <3 mm may be asymptomatic
Site: posterior horn of medial meniscus, junction of anterior horn + body of lateral meniscus
- cleft oriented perpendicular to free edge on AXIAL image:
- “truncated triangle” sign / “ghost meniscus” sign” ← tear through horn on COR view
- “cleft” sign ← tear through body on SAG view
- “marching cleft” sign
- blunting of the inner margin of meniscus (if image plane parallel to tear)
- poorly defined meniscus with diffusely increased SI (if tear extends to outer margin)
- usually seen on only 1 image = normal meniscus in adjacent sections
- discrete vertical focus of increased SI (if image plane perpendicular to tear)
Cx: lack of resistance to hoop stresses
Rx: frequently not repaired because of its location within avascular “white zone” → low likelihood of healing / regaining significant function
= radial-type tear
High association with: meniscal extrusion, particularly in MM
Incidence: increased if ACL tear present
- root should course over its respective tibial plateau on at least one COR image
- posterior root of MM should be detected just medial to PCL on SAG image (otherwise suspect root tear)
= combination of radial, horizontal, longitudinal components → frequent fragmentation of meniscus
Parrot Beak Tear
= free edge tear with vertical + horizontal component


Cause: usually degenerative
Site: in body of lateral meniscus near the junction of body + posterior horn
Free Meniscal Fragment
Flap Tear
= composite of radial tear that curves into longitudinal tear
Cause: traumatic, at times degenerative
Frequency: most common type of tear
N.B.: Search for displaced fragment in the absence of prior surgery / radial-type tear / severe underlying chondrosis if a foreshortened meniscus is present
Origin of flap: medial÷lateral meniscus = 7÷1
Site: common in midportion of medial meniscus
Location of displaced fragment:
- Medial meniscus
- posteriorly near / posterior to PCL (⅔)
- intercondylar notch / superior recess (⅓)
- Lateral meniscus
- posterior joint line (½)
- lateral recess (½)
- persistent pain, potential knee locking
- both horizontal and vertical components
- commonly extending to inferior surface of meniscus
Rx: partial meniscectomy
Bucket-handle Tear
= longitudinal vertical tear with attached unstable central migration of inner “handle” fragment
MR sensitivity: 60–88%
Cause: traumatic
Age: frequently in young individuals
Prevalence: 9–19% of symptomatic patients; 10% of all meniscal tears
Origin of handle flap: medial÷lateral meniscus = 7÷1
- locked knee, lack of full knee extension
- “absent bow-tie” sign (SAG image) = peripheral image fails to demonstrate normal bow-tie configuration on >2 consecutive images (71–98% sensitive, 63% specific)
DDx: radial tear of body, macerated meniscus, prior partial meniscectomy (in small / pediatric patient) - “fragment-in-notch” sign (COR image) = displaced fragment in intercondylar notch

- “double PCL” sign (SAG image) = medial meniscal fragment displaced into notch between PCL + medial tibial eminence oriented parallel to PCL (>98% specific, 27–53% sensitive, 93% PPV) ← intact ACL acts as barrier against further lateral displacement
DDx: ligament of Humphry (smaller and thinner, very close to PCL); oblique meniscomeniscal ligament, intercondylar osseous bodies - double anterior horn
- “flipped meniscus” sign
- disproportionately small posterior horn = hypoplastic / truncated anterior + posterior horns on sagittal image
- “double ACL” sign (LM) = fragment posterior to ACL
Rx: arthroscopic / surgical repair (reattachment / excision)
= surface irregularity along meniscal free edge without discrete tear
- loss of sharp tapered central edge
- subtle ill-defined horizontally oriented increased intrameniscal signal intensity contacting articular surface in posterior root
DDx: shallow partial-thickness tear / fraying / surrounding synovitis
= Peripheral Tear
= tearing of peripheral attachments of meniscus
- linear region of fluid separating meniscus from capsule
- uncovering of a portion of tibial plateau owing to inward movement of separated meniscus