Bone and Soft-Tissue Disorders

Frequency: 5% of all dislocations
- POSTERIOR HIP DISLOCATION (80–85%)
- Mechanism: classical dashboard injury (= flexed knee strikes dashboard)
- Associated with: fractures of posterior rim of acetabulum, femoral head
- adducted lower extremity flexed at hip
- ANTERIOR HIP DISLOCATION (5–10%)
- Mechanism: forced abduction + external rotation
- Associated with: fractures of acetabular rim, greater trochanter, femoral neck, femoral head (characteristic depression on posterosuperior and lateral portion)
- Subtypes:
- anterior obturator dislocation
- superoanterior / pubic hip dislocation
- lower extremity in external rotation
- prominent lesser trochanter
- obturator position of femoral head
- CENTRAL ACETABULAR FRACTURE-DISLOCATION
- Mechanism: force applied to lateral side of trochanter
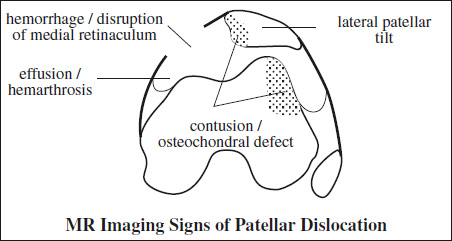
= TRANSIENT LATERAL PATELLAR DISLOCATION
Frequency: 2–3% of all knee injuries
Mechanism: during attempt to slow forward motion while pivoting medially on a planted foot; internal rotation of femur on fixed tibia while knee is flexed + quadriceps contraction produces a net lateral force; direct blow (rare)
At risk: patellar dysplasia (with flattened articular surface); shallow trochlear groove of femur; passive lateral hypermobility of patella; dysplastic distal ⅓ of vastus medialis obliquus muscle; nail-patella syndrome
Associated with: medial meniscal tear / major ligamentous injury in 31%
Age: 13–20 years (young physically active person); M <F
- 50–75% not clinically diagnosed initially ← self-reduction!
- lateral patellar tilt
- hemarthrosis (most common cause of hemarthrosis in young conscripts)
- concave impaction deformity of inferomedial patella (highly specific for prior patellar dislocation)
- medial parapatellar ossification ← chronic instability with repetitive stress to medial patellofemoral ligament
MR:
- “kissing” bone contusion / microfracture
- osteochondral injury of anterolateral femoral condyle + medial patellar facet (90% sensitive):
- intraarticular bodies (= avulsed osteochondral fragments of patella or lateral femoral condyle)
- increased SI with sprain / disruption / avulsion of medial patellar retinaculum + medial patellofemoral ligament + medial patellotibial lig.
- edema / hemorrhage within ± elevated vastus medialis obliquus muscle
- knee joint effusion = fluid depth >4 mm in suprapatellar recess (midline SAG image) or >10 mm in lateral recess (on lateral SAG image):
- hemarthros with fluid-fluid level (= sedimentation of blood components with low / intermediate T2 signal)
Rx:
- Temporary immobilization + rehabilitation: successful in 75%
- Surgery: fixation of osteochondral fragments if >1 cm2, medial capsule repair, lateral retinacular release, vastus medialis et lateralis rearrangement, medial retinaculum reefing
Sternoclavicular Dislocation (3%)
Posterior Sternoclavicular Dislocation
= posterior displacement of head of clavicle
Cause: blow to shoulder / medial clavicle
CECT confirms posterior sternoclavicular dislocation and may also disclose associated vascular injury.
Cx: injury to mediastinal blood vessels, trachea, esophagus
Anterior Sternoclavicular Dislocation
= anterior displacement of head of clavicle (more common but less serious type)
Cause: anterior blow to shoulder
- protruding clavicular head can be palpated
Cx: chronic pain, ankylosis, deformity
Rx: conservative therapy
Acromioclavicular Dislocation (12%)
Grade 1 (strain)
= stretching / partial tearing of acromioclavicular ligament fibers
- soft-tissue swelling
- stable AC joint without joint widening
Grade 2 (subluxation)
= disruption of acromioclavicular ligament + strain of coracoclavicular ligament
- elevation of clavicle of <100% of shaft width (weight-bearing!)
- widening of AC joint
Grade 3 (superior dislocation)
= disruption of acromioclavicular + coracoclavicular ligg.
- widening of AC joint
- elevation of clavicle >100% of shaft width
Grade 4 (posterior dislocation)
- posterior position of clavicle with respect to acromion
Grade 5 (fascial injury)
- penetration of clavicle through deltotrapezial fascia
Grade 6 (inferior dislocation)
- inferior position of clavicle with respect to acromion
Glenohumeral Dislocation (85%)
- Glenohumeral joint dislocations make up >50% of all dislocations!
Anterior / Subcoracoid Shoulder Dislocation
(85–95–98% of all shoulder dislocations)
Prevalence: up to 2% in general population
Types: subcoracoid, subglenoid, subclavicular, intrathoracic
Mechanism: external rotation + abduction (fall on outstretched arm); direct posterior blow in contact sport / forced ABER position)
Age: in younger individuals in their teens
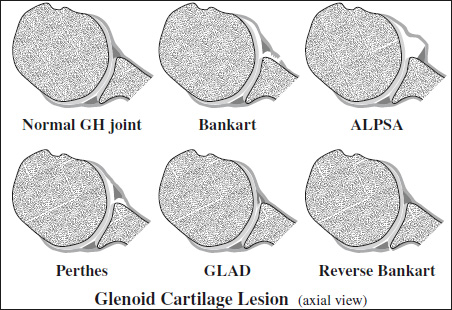
- Bankart lesion = anterior capsulolabral avulsion
[Arthur Sydney Blundell Bankart (1879–1951), British orthopedic surgeon]
= detachment of glenoid labrum and joint capsule from anterior glenoid rim during anterior shoulder dislocation- detachment of anterior inferior glenohumeral labroligamentous complex (IGHLC = anterior-inferior glenoid labrum including labral insertion of inferior glenoid ligament) from glenoid at 3 to 6 o'clock position (= cartilaginous Bankart)
- lifted disrupted scapular periosteum
- labrum floats in anterior joint space
- Soft Bankart
- no bony avulsion
- Osseous Bankart
- fracture of anterior rim of glenoid
Shoulder instability increases with increasing size of the Bankart fragment. The redislocation rate is higher when the fragment involves >20–25% of the glenoid surface area. A concomitant Hill-Sachs lesion reduces stability even further.
May be associated with:- fracture of greater tuberosity (15–35%)
- fracture of coracoid process (3–13%)
- Hill-Sachs defect / deformity (25–50–81%)
- = depression / impacted fracture of posterolateral surface of humeral head at / above level of coracoid process ← impaction against anterior edge of glenoid rim in subglenoid type
- [Harold Arthur Hill (1901–1973) and Maurice David Sachs (1909–1987), radiologists in San Francisco]
- Perthes lesion (variant of Bankart)
- easily overlooked on MR / arthroscopy → best detected in ABER position with traction on IGHL
- labrum separated from articular cartilage
- scapular periosteum stripped medially but with intact periosteal sleeve
- nondisplaced avulsed labrum (DDx to ALPSA)
- Glenoid Labrum Articular Disruption (GLAD)
= combination of labral tear + cartilage defect- complete avulsion of anteroinferior glenoid labrum
- small fragment of articular cartilage also detached
- chondral flaps best visualized on MR arthrogram
- Humeral Avulsion of the Glenohumeral Ligament (HAGL) = failure at humeral attachment site
Prevalence: 52% in acute trauma; 2–9% of anterior glenohumeral instabilities
Age: 28 (range, 12–54) years; M÷F = 92÷8- “J / reversed J” sign (for RT / LT shoulder)
= detached end of anterior / posterior band of IGHL that falls inferiorly away from neck of humerus- extravasation of joint effusion / contrast material at the humeral insertion of disrupted capsule
Bony HAGL- avulsion of humeral cortex along with IGHL
- Anterior Labroligamentous Periosteal Sleeve Avulsion (ALPSA) = medialized Bankart
- best detected in ABER position
- complete avulsion of anteroinferior glenoid labrum
- avulsed scapular periosteum intact
- labroligamentous complex rolls up + becomes displaced medially + inferiorly
- recurrent anterior humeral dislocations ← incompetent anterior band of IGHL
- can heal into a deformed labrum → difficult to diagnose
- Reverse Bankart
Prevalence: 2–4% of all shoulder instability
Mechanism: excessive force applied to adducted and internally rotated shoulder ← swimming, throwing, punching, convulsion- posterior labral tear
MRI (arthrography improves sensitivity to 89–99% and specificity to >90%):
- hemorrhagic effusion (in acute injury)
- increased SI in anterior-inferior labrum + capsule (DDx: magic angle artifact)
- discrete tear / fragmentation of labrum
- ± tear of middle glenohumeral ligament
- tear of degenerated supraspinatus tendon (in 33% of patients >40 years of age)
- tear of degenerated subscapularis tendon (in 33% of patients >40 years of age)
- myotendinous subscapularis strain / contusion
- paralabral cysts are usually associated with labral tears; may cause denervation of suprascapular nerve simulating impingement syndrome (DDx: age-related degeneration)
Prognosis: significance of glenoid rim fracture is greater than of Hill-Sachs fracture
Cx:
- Recurrent dislocations: inversely related to age (83% <20 years; 16% >40 years of age); M÷F = 3÷1
- Repeated dislocations ← incomplete / inadequate healing = chronic recurrent anterior shoulder instability
- Arthritis (with repeated subluxations)
Rx:
- Conservative treatment for most
- Surgical fixation for young athletes
Posterior Shoulder Dislocation (2–5%)
Cause:
- traumatic: convulsive disorders /electric shock therapy
- nontraumatic: voluntary, involuntary, congenital, developmental
Types: subacromial, subglenoid, subspinous
- In >50% unrecognized initially + subsequently misdiagnosed as frozen shoulder!
- Average interval between injury and diagnosis is 1 year!
- “rim” sign (66%) = distance between medial border of humeral head + anterior glenoid rim <6 mm
May be associated with:
- “trough” sign (75%) = “reverse Hill-Sachs”
= compression fracture of anteromedial humeral head (tangential Grashey view of glenoid!) - fracture of posterior glenoid rim
- avulsion fracture of lesser tuberosity
MRI:
- tear of subscapularis tendon
- empty bicipital groove (= dislocated bicipital tendon)
Inferior Shoulder Dislocation (0.5%)
= LUXATIO ERECTA
= extremity held over head in fixed position with elbow flexed
Mechanism: severe hyperabduction of arm resulting in impingement of humeral head against acromion
- humeral articular surface faces inferiorly
Cx: rotator cuff tear; fracture of acromion ± inferior glenoid fossa ± greater tuberosity; neurovascular injury
Superior Shoulder Dislocation (<1%)
= humeral head driven upward through rotator cuff
May be associated with: fracture of humerus, clavicle, acromion
DDx: drooping shoulder (transient phenomenon after fracture of surgical neck of humerus ← hemarthrosis / muscle imbalance)
Gadolinium Shoulder Arthrography
- fluoroscopically guided needle insertion from an anterior approach
- confirmation of needle placement with iodinated contrast material
- injection of 12–20 mL of diluted gadolinium chelate solution:
- 0.1 mL of gadolinium DTPA (469 mg/mL) into
- 20 mL of bacteriostatic saline
- patient's arm and shoulder are moved through full range of motion
= total + permanent loss of contact between tendon and bicipital groove
Types:
- dislocation inside subscapularis tendon leaving anterior fascia intact
- intraarticular dislocation with complete tear of all insertions on lesser tuberosity but intact anterior fascia (lesion hidden in joint space)
- intraarticular dislocation with complete tear of all insertions on lesser tuberosity + anterior fascia
- dislocation over intact subscapularis tendon (= rupture of the supraspinatus tendon and CHL)
Associated with: tears of ligamentous pulley
Location: intraarticular extrasynovial (within reflection of synovial membrane)
MR:
- dislocated biceps tendon medial to empty bicipital groove (axial image)
- variably increased signal intensity
- thickening, flattening, broadening of the tendon
- fluid around displaced biceps tendon
Biceps Tendon Subluxation
= partial / transitional loss of contact between biceps tendon + bicipital groove
Direction:
- intraarticular
- between subscapularis tendon and CHL
- external to CHL
- intrasheath
Mechanism: fall on outstretched hand
Frequency: 10% of all carpal injuries
◊Up to 25% overlooked at initial examination!
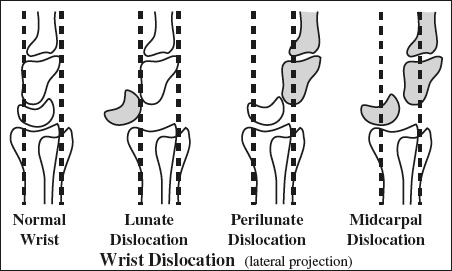
Lunate Dislocation
= final stage of perilunate injury with highest degree of instablity
- “spilled teacup” sign = lunate dislocated in volar direction (on LAT view)
- rest of carpus assumes alignment with radius
Perilunate Dislocation
= dislocation of capitate head from concavity of distal lunate
Prevalence: 2–3 times more common than lunate dislocation
Mechanism: high-energy wrist hyperextension (MVC, fall from height, sports) with sequential injury of scapholunate → lunocapitate → lunotriquetral joints → complete dislocation
Average age: 30 years; M >>F
Associated with: fracture in 75%
- disruption of carpal arcs (AP view)
- Terry-Thomas sign = widening of space between scaphoid and lunate (AP view)
- triangular lunate (AP view)
- posterior dislocation of capitate head relative to lunate (LAT view)
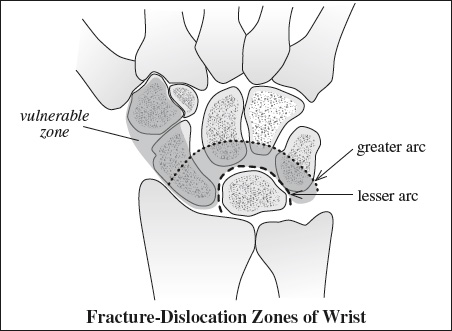
Greater Arc Injury
= perilunate dislocation + fracture of scaphoid / trapezium / capitate / hamate / triquetrum
- Twice as common as lesser arc injury
- Most commonly transscaphoid perilunate dislocation
- fracture of any carpal bone around lunate
Lesser Arc Injury
= pure ligamentous disruption around lunate
- most commonly dorsal dislocation
Rx: open reduction + internal fixation
Rotary Subluxation of Scaphoid
= Scapholunate dissociation
= tearing of interosseous ligaments of lunate, scaphoid, capitate
Mechanism: acute dorsiflexion of wrist; may be associated with rheumatoid arthritis
- gap >4 mm between scaphoid + lunate (PA view)
- foreshortening of scaphoid
- “ring” sign of distal pole of scaphoid