section name header
Images
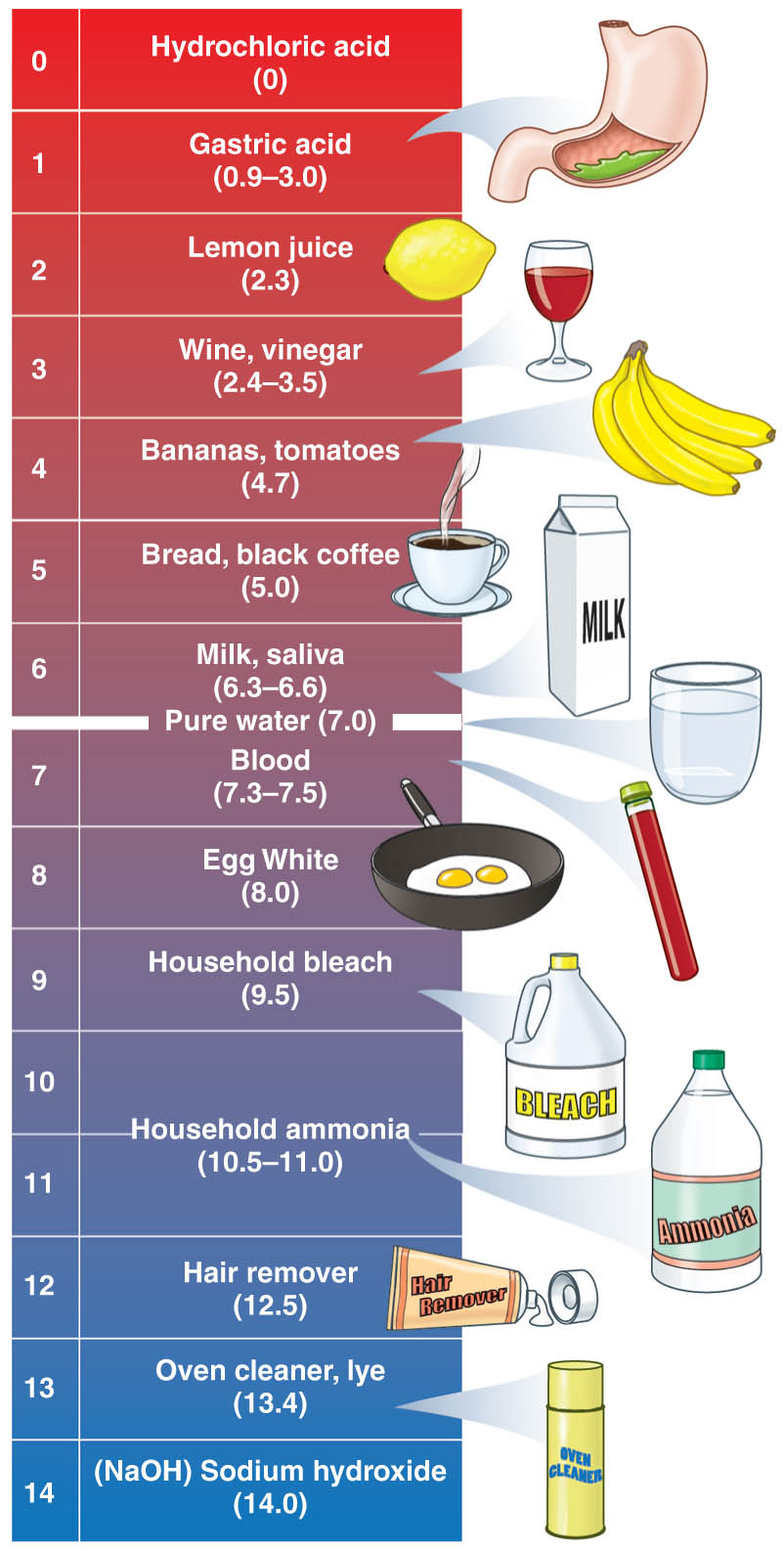
Values of body fluids and some familiar solutions