section name header
Image
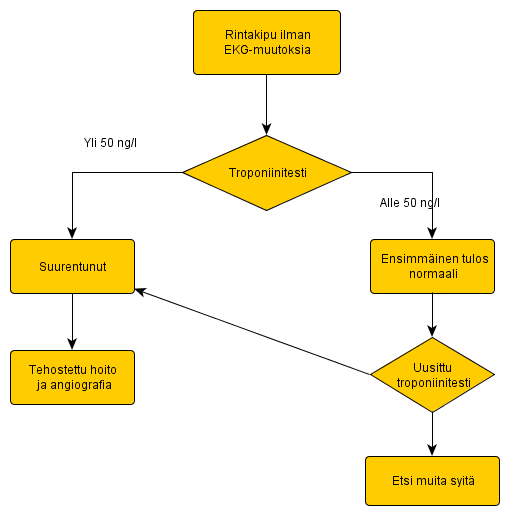
Rintakipu Ilman Ekg-Muutoksia
Yksinkertainen kaavio rintakivun selvittämiseen.