section name header
Image
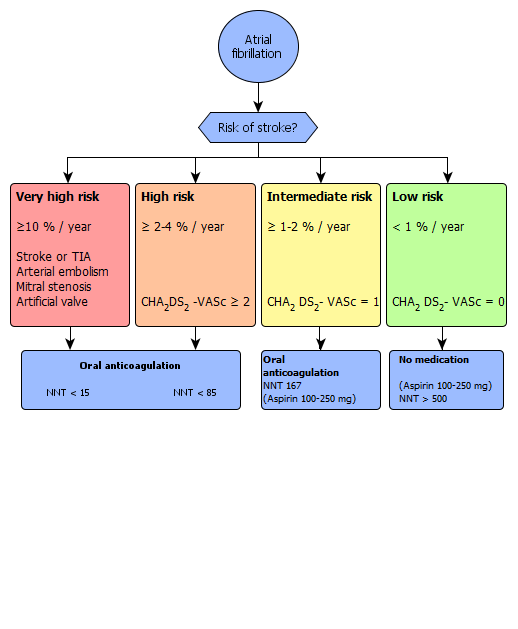
Anticoagulation for Atrial Fibrillation