Tendon Ruptures of the Biceps Muscle
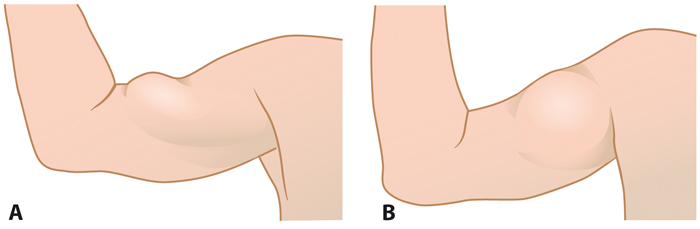
Tendon ruptures of the biceps muscle. A: Proximal long head tendon rupture with distal retraction of the biceps muscle belly. B: Distal tendon rupture with proximal retraction of the biceps muscle belly.
Picture: Duodecim Medical Publications Ltd., text: Anssi Ryösä, Juha Kukkonen ja Kaisa Lehtimäki
Primary/Secondary Keywords
- biceps
- biceps muscle
- tendon rupture
- tendon
- rupture
- biceps brachii muscle
- coracoid process
- proximal tendon
- proximal rupture
- distal tendon
- distal rupture
- long head
- short head
- Popeye
- Popeye muscle
- biceps rupture