Image
Anemia

Hemoglobiinin viitearvot
- Naiset 117-155 g/l, miehet 134-167 g/l
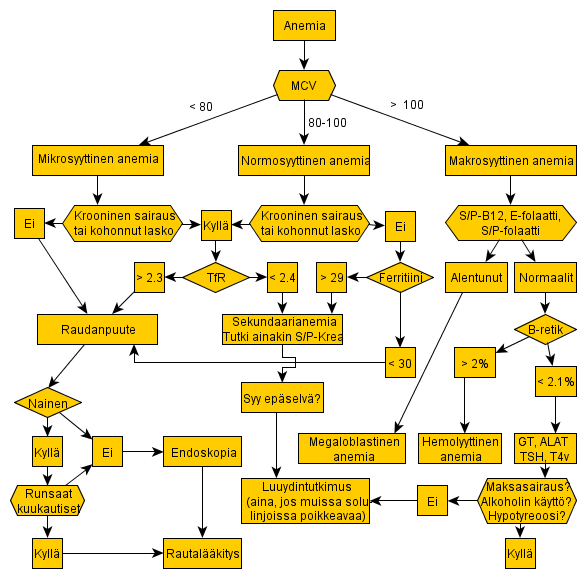
Anemioiden jaottelu punasolukoon mukaan
- Mikrosyyttiset anemiat: raudanpuuteanemia, sekundaarianemia, talassemia
- Normosyyttiset anemiat: sekundaarianemia, hemolyyttinen anemia, akuutti vuoto, aplastinen anemia, luuydininfiltraatit
- Makrosyyttiset anemiat: B12-vitamiinin tai folaatin puutos, verenhukka (> 2 vrk), maksasairaus, alkoholin suurkulutus, myelodysplasia ja pahanlaatuiset veritaudit, hypotyreoosi
Raudanpuuteanemia
- Raudanpuuteanemia on oire, jonka takaa tulee etsiä varsinainen diagnoosi.
- Raudanpuute fertiili-iän ohittaneilla naisilla ja kaikilla miehillä on aina poikkeavaa.
- Jos potilaalla on mikrosyyttinen anemia ja sekundaarianemian mahdollisuus tuntuu epätodennäk�iseltä, on raudanpuuteanemia hyvin todennäk�inen.
- Lisätutkimukset:
- S/P-Ferrit < 30 µg/l merkitsee raudanpuutetta. Normaali tai kohonnut arvo voi selittyä tulehdusreaktiolla (ferritiini on akuutin faasin reaktantti) eikä sulje pois raudanpuutetta potilaalla, jonka CRP tai La on koholla.
- Raudanpuute kroonisen sairauden yhteydessä todetaan määrittämällä liukoisen transferriinireseptorin pitoisuus (P-TfR). Arvo > 2.3 mg/l viittaa vahvasti raudanpuutteeseen.
- Raudanpuutteen syytä on kaikilta miehiltä ja niiltä naisilta, joiden kuukautisvuoto ei selitä anemiaa, etsittävä suoliston endoskopiatutkimuksilla.
- Kaikkien yli 50-vuotiaiden paksusuoli on syytä tutkia kolonoskopialla.
- Nuoremmalle potilaalle tehdään ensin gastroskopia, etenkin jos potilaalla on ylävatsaoireita.
Sekundaarianemia
- Kroonisen sairauden anemia: krooniset infektiot ja muut tulehdussairaudet, pahanlaatuiset kasvaimet
- Elinspesifiset syyt: tavallisimmat krooninen munuaisten vajaatoiminta, maksasairaudet
- Perustutkimukset: PVK, La, CRP
- Luuydintutkimus aiheellinen kaikissa epäselvissä tapauksissa
Megaloblastianemia
- Epäile megaloblastianemiaa, jos potilaalla on makrosyyttinen anemia (E-MCV on korkea).
- Selvitä megaloblastianemian etiologia (tavallisesti B12-vitamiinin tai folaatin puute).
- Esitiedot ravinnosta ja ruoansulatuskanavasta oleellisia
- Määritä S/P-B12-Vit , fS/fP-Folaat ja fE-Folaat.
- B12-vitamiinin puute: atrofinen gastriitti, ohutsuolen loppuosan taudit, lapamato
- Folaatin puute: puutteellinen ravinto (alkoholistit), suurentunut tarve (raskaus, keskosuus, hemolyysi, sy�päsairaus), malabsorptio (keliakia), kasvanut menetys (eräät ihotaudit, maksasairaus ja dialyysi), monet lääkeaineet
Hemolyyttinen anemia
- Yleisin suomalaisella väest�llä on autoimmuunihemolyyttinen anemia AIHA; 1 uusi tapaus 75 000 henkeä kohti vuodessa.
- Maailmanlaajuisesti hemolyyttiset anemiat ovat hyvin yleisiä ongelmia (sirppisoluanemia, talassemiat, poikkeavat hemoglobiinit).
- Selvittelyssä PVK:n lisäksi keskeinen on retikulosyyttien tutkiminen. Normaali E/B-Retik sulkee yleensä pois hemolyysin.