Image
Lääkkeiden Valinta

Verenpainelääkkeen valinta
- Lääke on valittava yksilöllisesti.
- Valintaan vaikuttavia tekijöitä ovat
- kohonneen verenpaineen vaikeusaste
- kohonneeseen verenpaineeseen liittyvät elinvauriot
- muut samanaikaiset riskitekijät, sairaudet ja lääkitykset
- lääkehoidon kustannukset.
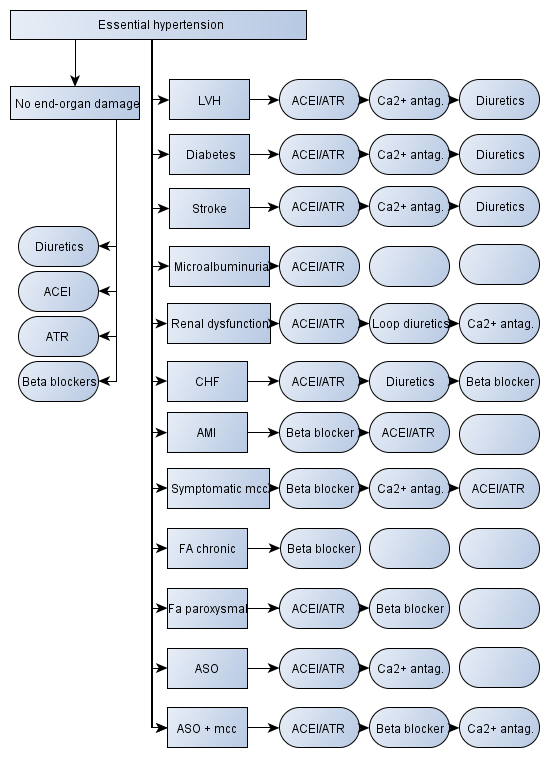
- Kaaviossa on ehdotus verenpainelääkkeen valinnasta eri sairaustiloissa ja erityistilanteissa.
- Lääkkeiden järjestys rivillä on niiden suosituimmuusjärjestys.
Kaavion käyttö sähköisen potilaskertomuksen yhteydessä
- Potilaskertomustiedoista löytyvät sairaudet ja riskitekijät on merkitty sinisellä kehyksellä.
- Potilaskertomuksen perusteella käytössä olevat lääkkeet on merkitty sinisellä kehyksellä.
- Ehdotus seuraavaksi lisättävästä lääkkeestä on merkitty vihreällä kehyksellä.
- Jos potilaalla on useita lääkevalintaan vaikuttavia sairauksia tai riskitekijöitä, voivat vihreällä merkityt ehdotukset sisältää eri lääkkeitä. Tällöin tulee käyttää kliinistä harkintaa ja valita lääke, jonka hyötyjen ja haittojen suhde on edullisin.