Scarred Leucoderma on the Face
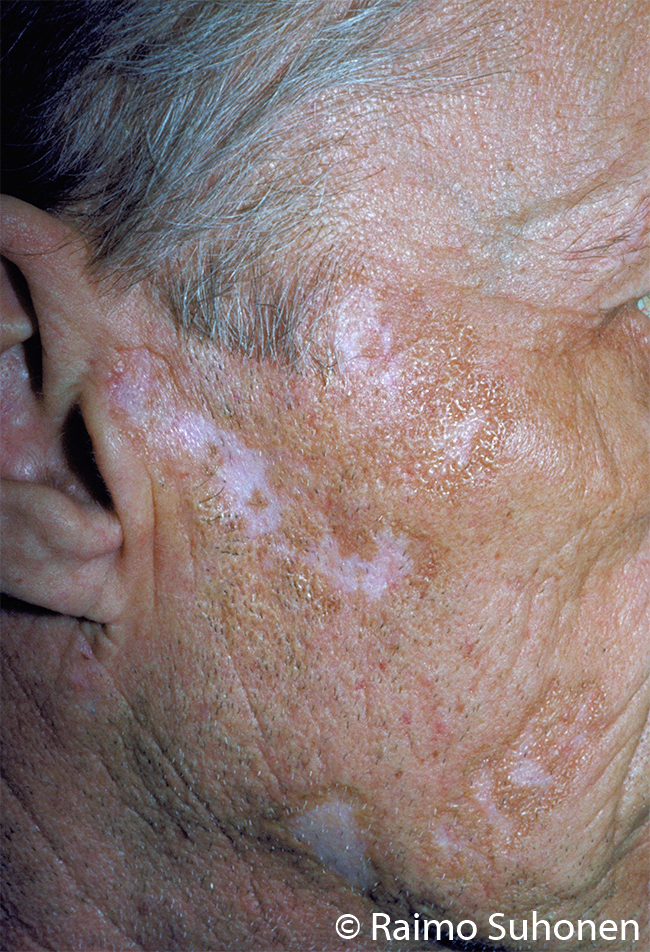
Scarred leucoderma on the face. While healing, discoid lupus erythematosus leaves a light scar, the development of which can usually be prevented by early, active treatment.
Picture and text: Raimo Suhonen
Primary/Secondary Keywords