Selecting Anticoagulant Therapy in Atrial Fibrillation
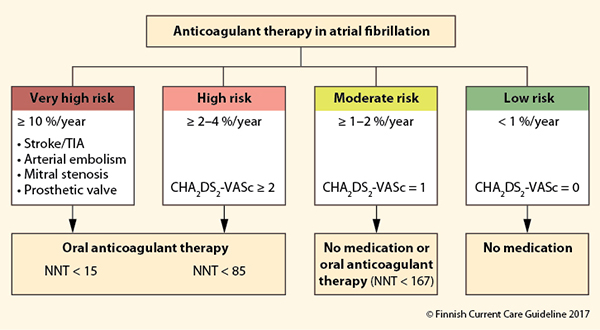
The justification of anticoagulant therapy is assessed in relation to the patient's individual risk of stroke using the (modified1 ) CHA2DS2-VASc risk score. In high-risk patients (CHA2DS2-VASc HASH(0x2fcfe80) 2), anticoagulant therapy (direct anticoagulant or warfarin) is indicated almost without exception. In patients with moderate risk (CHA2DS2-VASc = 1), the need for anticoagulation is assessed individually. Anticoagulation may be omitted, if the bleeding risk is high, the patient does not want to use anticoagulant therapy, the risk factor (e.g. hypertension) is well managed and the patient does not have other, smaller risk factors (e.g. smoking, dyslipidaemia, renal failure). Anticoagulation therapy is not given to low-risk patients (CHA2DS2-VASc = 0), since in such patients its adverse effects exceed its benefits. ASA and ADP receptor antagonists are not suitable for the prevention of thrombosis associated with atrial fibrillation, due to their poor efficacy and adverse effects. The NNT (number needed to treat) indicates the number of patients that need to be treated so that one of them avoids stroke during one year, compared with those using placebo. If needed, the anticoagulation therapy may be temporarily discontinued during such procedures or surgery that entail bleeding risk, with the exception of highest-risk patients.
1 In this modified version of the score, female sex gives one point only if age is HASH(0x2fcfe80) 75 years, allowing the use of identical cut-off values for both men and women. For more details, see Table 1 in article Indications for and Implementation of Anticoagulant Therapy in Atrial Fibrillation.
Picture: Finnish Current Care Guidelines
Primary/Secondary Keywords
- Internal medicine
- Cardiology
- Atrial fibrillation
- AF
- Anticoagulation
- Oral anticoagulation
- Anticoagulation, oral
- Anticoagulant
- Anticoagulants
- Warfarin
- CHA2DS2-VASc
- Risk score
- Stroke risk