Evaluation of ECG ST Segment Depression in an Exercise Stress Test
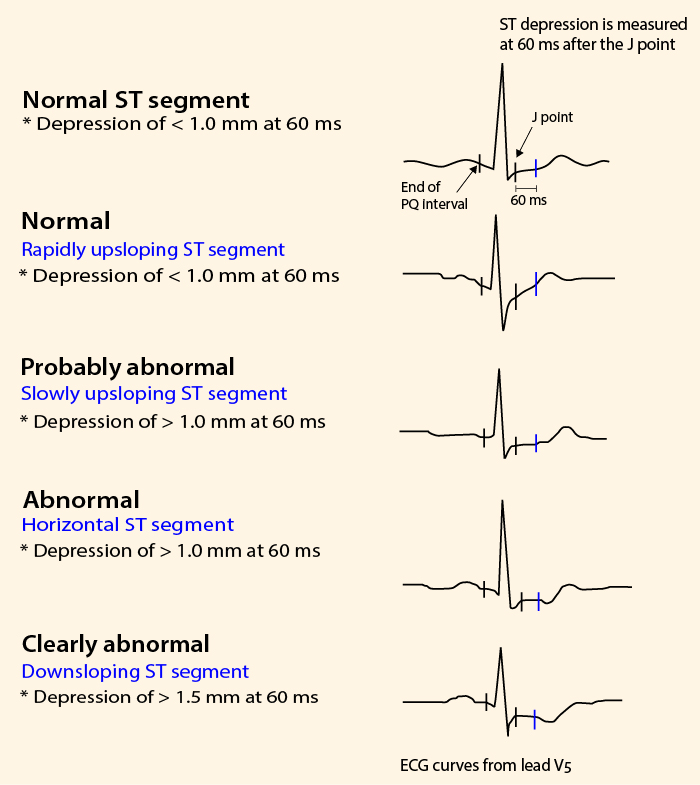
Evaluation of ECG ST segment depression in an exercise stress test. The change in ST segment is measured at 0.06 s (blue line) after the J point, or at J+0.08 s if the heart rate is < 130/min. The level at the end of the PQ interval is used as the reference level.
Kuva ja teksti: Jari Laukkanen
Primary/Secondary Keywords
- ECG
- ST segment
- ST segment depression
- clinical stress test
- J-point
- J point
- exercise stress test
- stress test
- stress ECG