section name header
Image
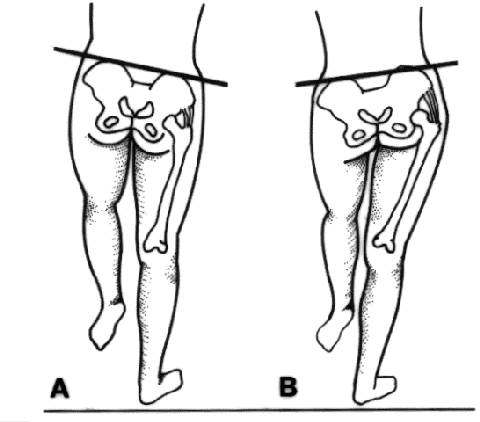
Trendelenburg's Test
Trendelenburg's test.
Primary/Secondary Keywords
Physiatry
Neurology
status
clinical examination
muscle weakness
Trendelenburg's test
Trendelenburg sign