Population: Adults with symptomatic or asymptomatic AAA.
Organizations
 ACC/AHA 2022, NICE 2020, ESC 2014
ACC/AHA 2022, NICE 2020, ESC 2014
Recommendations
–Offer surveillance without intervention if AAA diameter <5.5 cm in men and <5.0 in women.
–In patients with stable small AAA, monitor with imaging at the following frequencies:
• Every 3 y for AAA 3–3.9 cm diameter.
• Every year for AAA 4.0–4.9 cm diameter in men.
• Every year for AAA 4.0–4.4 cm diameter in women.
• Every 6 mo for AAA 4.5–5.0 cm diameter.
–In patients with bicuspid aortic valve (BAV), perform TTE to evaluate aortic root, ascending aorta. Repeat imaging should be based on the above parameters.
–In patients with Marfan syndrome, Loeys-Diets syndrome, perform TTE at the time of diagnosis and 6 mo afterward to check for diameter stability. Perform TTE annually if stable.
–Target modifiable risk factors. No non-surgical interventions reliably prevent AAA from growing.
• Smoking is a risk factor for rupture. Provide cessation counseling and medications to all patients with AAA, as cessation slows the growth. Duration of smoking is more significant than quantity smoked.
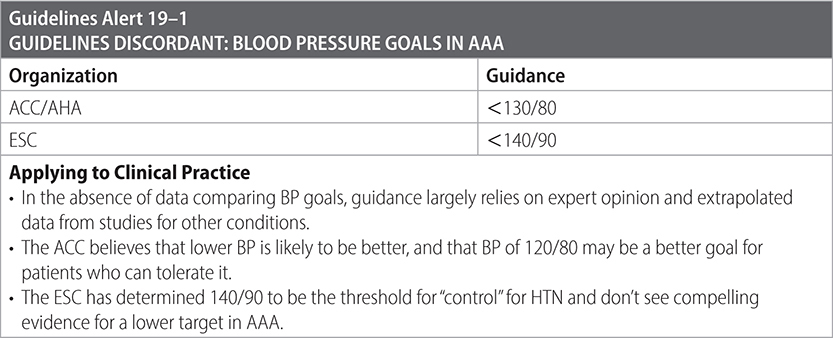
• HTN is a risk factor for AAA rupture. Use beta-blockers as first-line treatment if HTN is a comorbid condition.
• Treat other modifiable risk factors for expansion (CAD, PAD, HLD) as usual with guideline-directed medical therapy.
–Nonmodifiable risk factors include size of aneurysm, age, female sex, cardiac/renal transplant.
–Consider statins and ACE-inhibitors to reduce complications.
–Consider beta-blockers to reduce the rate of growth. (ACC)

Surgical Therapy
–Indication for repair:
• Symptomatic.
• Asymptomatic > 4.0 cm in diameter growing >1 cm/y.
• Asymptomatic and ≥5.5 cm in diameter.
–Indication for referral urgency:
• If symptomatic but nonruptured, urgent referral to vascular specialist.
• If asymptomatic >5.5 cm, see vascular specialist within 2 wk.
• If asymptomatic 3.0–5.4 cm, see vascular specialist within 3 mo.
–Repair ruptured AAA emergently. Consider TXA to slow blood loss.
Practice Pearl
• Studies of beta-blockers and rate of expansion have produced contradictory data. 2013 ESC HTN guidelines suggest using them as first line for HTN and AAA, but data do not strongly support their use outside of HTN.
Risk Factors for Developing AAA
• Age > 60 y. About 1 person in 1000 develops an AAA between the ages of 60 and 65.
• Smoking. The risk is directly related to the number of years smoking and decreases in the years following smoking cessation.
• Men develop AAA 4–5 times more often than women.
• Ethnicity. More common in the White population.
• History of CHD, PAD, HTN, and hypercholesterolemia.
• Family history of AAA. Accentuates the risks associated with age and sex. The risk of developing an aneurysm among brothers of a person with a known aneurysm who are >60 y of age is as high as 18%.
Risk Factors for AAA Expansion
• Age > 70 y, cardiac or renal transplant, previous stroke, severe cardiac disease, tobacco use.
Risk Factors for AAA Rupture
• Aneurysms expand at an average rate of 0.3–0.4 cm/y.
• The annual risk of rupture based upon aneurysm size is estimated as follows:
– <4.0 cm diameter = <0.5%.
– Between 4.0 and 4.9 cm diameter = 0.5%–5%.
– Between 5.0 and 5.9 cm diameter = 3%–15%.
– Between 6.0 and 6.9 cm diameter = 10%–20%.
– Between 7.0 and 7.9 cm diameter = 20%–40%.
– ≥8.0 cm diameter = 30%–50%.
• Aneurysms that expand rapidly (>0.5 cm over 6 mo) are at high risk for rupture.
• Growth tends to be more rapid in smokers and less rapid in patients with peripheral artery disease or diabetes mellitus.
• The risk of rupture of large aneurysms (≥5.0 cm) is significantly greater in women (18%) than in men (12%).
• Other risk factors for rupture: cardiac or renal transplant, decreased forced expiratory volume in 1 s, higher mean BP, larger initial AAA diameter, current tobacco use.
Sources
–ACC/AHA. Aortic Disease Guideline for the Diagnosis and Management of Aortic Disease. 13 December 2022.
–NICE guidelines 156. Abdominal aortic aneurysm: diagnosis and management. 19 March 2020.
–J Vasc Inter Radiol. 2006;17:1383-1398.
–Eur Heart J. 2014;35:2873-2926.