Urinary excretion of high-dose methotrexate (MTX) and effect of medications and urine pH.
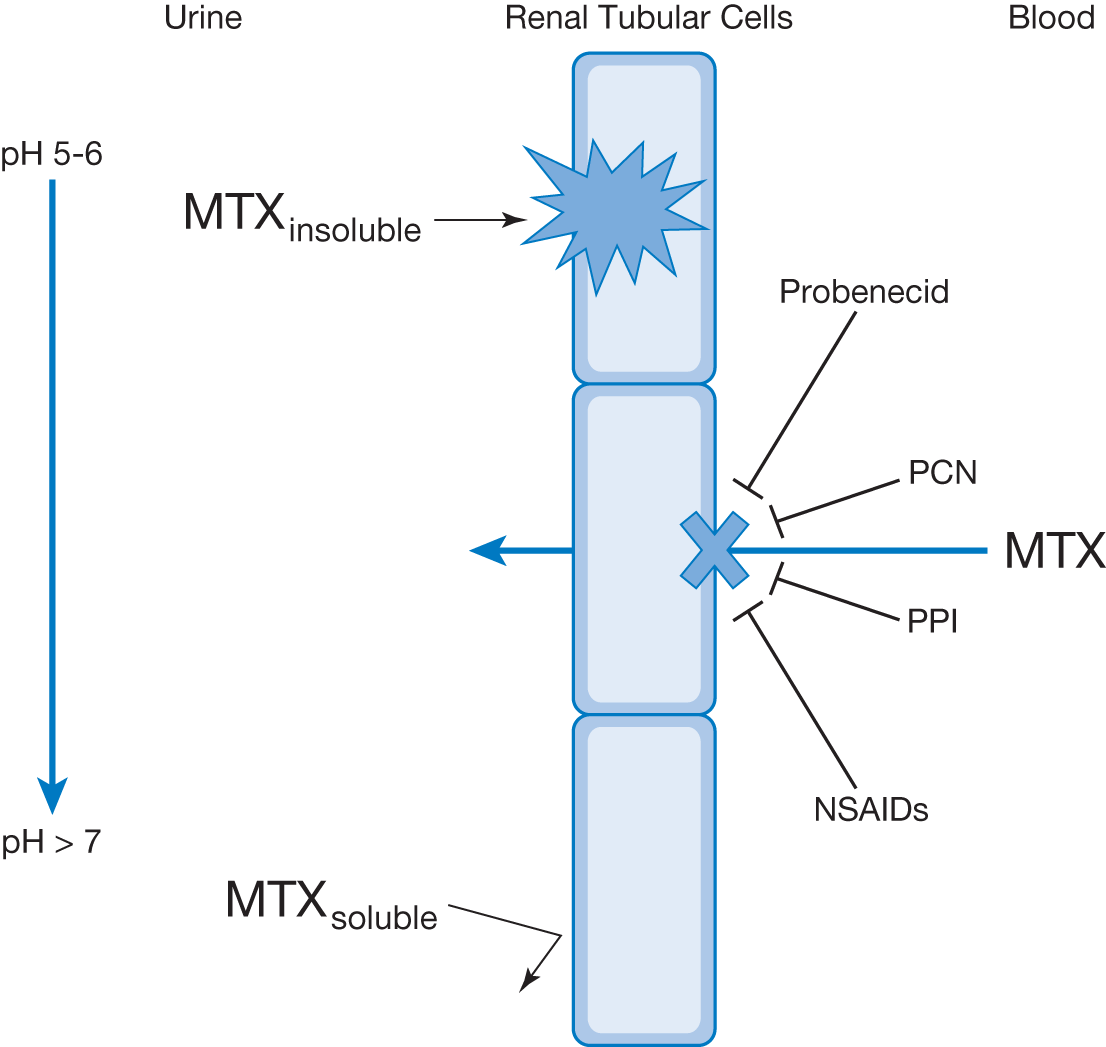
Acute kidney injury is another directly preventable toxicity of high-dose MTX therapy. Administration strategies to prevent this toxicity include hyperhydration and alkalization of urine with IV solutions containing sodium bicarbonate. MTX, is a di (i.e., 2)-carboxylic acid and its metabolites are poorly soluble at an acidic pH. To prevent crystallization within the renal tubules during elimination, alkalization of urine pH to >7 significantly increases MTX solubility and , therefore, prevents precipitation and deposition of MTX into the renal tubules. Due to this increased risk of kidney injury, high-dose MTX must never be given in a patient with urine pH of <7. Several medications also affect active secretion of MTX into the urine and should be avoided during high-dose MTX clearance; these include penicillins (PCN), nonsteroidal anti-inflammatory drugs (NSAIDs), probenecid, and proton pump inhibitors (PPIs).