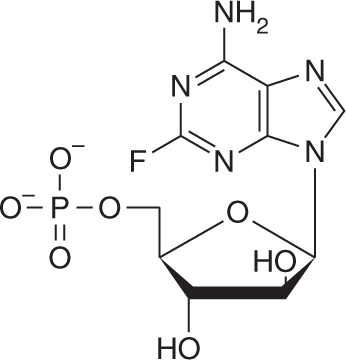
5'-Monophosphate analog of arabinofuranosyladenosine (F-ara-A) with high specificity for lymphoid cells. Presence of the 2-fluoro group on adenine ring renders fludarabine resistant to breakdown by adenosine deaminase.
Considered a prodrug and inactive in its parent form. Following administration, it is rapidly dephosphorylated to 2-fluoro-ara-adenosine (F-ara-A). F-ara-A enters cells via a nucleoside transport system and is then phosphorylated first to its monophosphate form and eventually to the active 5'-triphosphate metabolite (F-ara-ATP).
Antitumor activity against both dividing and resting cells.
Triphosphate metabolite incorporates into DNA, resulting in inhibition of DNA chain extension.
Inhibition of ribonucleotide reductase by fludarabine triphosphate.
Inhibition of DNA polymerase-α and DNA polymerase-β by the triphosphate metabolite, resulting in inhibition of DNA synthesis and DNA repair.
Induction of apoptosis (programmed cell death).
Decreased expression of the activating enzyme, deoxycytidine kinase.
Decreased nucleoside transport of drug into cells.
Orally bioavailable, in the range of 50%-65%, and an oral tablet form is available. Absorption is not affected by food.
Recommended dose is 25 mg/m2 IV on days 1-5 every 28 days.
For oral usage, the recommended dose is 40 mg/m2 PO on days 1-5 every 28 days.
Cytarabine—Fludarabine may enhance the antitumor activity of cytarabine by inducing the expression of deoxycytidine kinase.
Cyclophosphamide, cisplatin, mitoxantrone—Fludarabine may enhance the antitumor activity of cyclophosphamide, cisplatin, and mitoxantrone by inhibiting nucleotide excision repair mechanisms.
Use with caution in patients with abnormal renal function. Dose reduction is not required for CrCl >80 mL/min. For CrCl between 50 and 79 mL/min, the dose should be reduced to 20 mg/m2, and for CrCl between 30 and 49 mL/min, the dose should be reduced to 15 mg/m2. Fludarabine should not be administered to patients with CrCl <30 mL/min.
Use with caution in elderly patients and in those with bone marrow impairment, as they are at increased risk of toxicity.
Monitor for signs of infection. Patients are at increased risk for opportunistic infections, including herpes, fungi, and PJP. Patients should be empirically placed on trimethoprim/sulfamethoxazole prophylaxis, 1 DS tablet PO bid 3 times/week.
Monitor for signs of tumor lysis syndrome, especially in patients with a high tumor cell burden. May occur as early as within the first week of treatment.
Allopurinol may be given prior to initiation of fludarabine therapy to prevent hyperuricemia.
Use irradiated blood products in patients requiring transfusions, as transfusion-associated graft-versus-host disease can occur rarely after transfusion of non-irradiated products in patients treated with fludarabine.
Used as part of an immunosuppressive lymphodepletion conditioning regimen with cyclophosphamide in adoptive immunotherapy and chimeric antigen receptor (CAR) T-cell therapy.
Pregnancy category D. Breastfeeding should be avoided.
Myelosuppression is dose-limiting. Neutrophil nadir occurs in 10-13 days, with recovery by day 14-21. Autoimmune hemolytic anemia and drug-induced aplastic anemia can also occur.
Immunosuppression. Decrease in CD4 and CD8 T cells occurs in most patients. Increased risk of opportunistic infections, including fungus, herpes, and PJP. Recovery of CD4 count is slow and may take over a year to return to normal.
Nausea and vomiting are usually mild.
Fever occurs in 20%-30% of patients. Most likely due to release of pyrogens and/or cytokines from tumor cells. Associated with fatigue, malaise, myalgias, arthralgias, and chills.
Hypersensitivity reaction with maculopapular skin rash, erythema, and pruritus.
Tumor lysis syndrome. Rarely seen (in less than 1%-2% of patients) and most often in the setting of high tumor-cell burden.
Transient elevation in serum transaminases. Clinically asymptomatic.