Rx:
Surgery by age 1 yr; does not decrease CA risk (Cancer 1982;49:1023) or survival (Peds 1996;97:590) but improves fertility and facilitates self-exam. Swedish study finds surgery before puberty (13 yr) still has 2.25% relative risk incr but after 13, risk incr × 5+%
Hormonal rx with HCG or GnRH not much help (Nejm 1986;314:466, 510)
Educate teenagers to do careful testicular self-exam
Figure 13.2 Interpretation of the Assay of Serum Müllerian Inhibiting Substance in the Evaluation of Boys with Bilateral Undescended Testes or Children with Intersexual Disorders
Boys with Bilateral Undescended Testes (Normal Phallus) 
Children with intersexual Disorders (Ambiguous Genitalia)
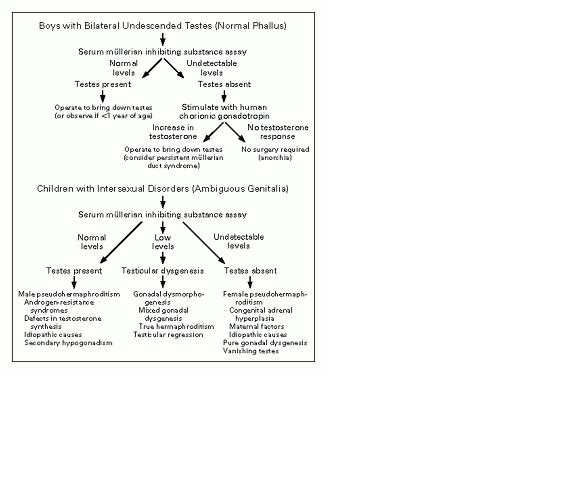
Reproduced with permission from Lee MM, et al. Measurements of serum mullerian inhibiting substance in the evaluation of children with nonpalpable gonads. New Eng J Med 1997:336:1480. Copyright 1997 Mass. Medical Society, all rights reserved.