| When T is… | and N is… | and M is… | Then the stage group is… |
|---|---|---|---|
| Tis | N0 | M0 | 0 |
| T1 | N0 | M0 | IA |
| T2a | N0 | M0 | IB |
| T2b-c, T3 | N0 | M0 | IIA |
| T4 | N0 | M0 | IIB |
| Any T | N1 | M0 | IIIA |
| Any T | N2 | M0 | IIIB |
| Any T | Any N | M1 | IV |
Cancers Staged Using This Staging System
All primary carcinomas of the eyelid, including basal cell carcinoma (BCC), squamous cell carcinoma (SCC), sebaceous carcinoma, and other rare carcinomas, such as all varieties of sweat gland carcinoma (e.g., eccrine carcinoma), are classified using this staging system.
Cancers Not Staged Using This Staging System
Carcinomas of the head and neck region from another anatomic site (other than the eyelids and orbital area) but that secondarily extend to the eyelids should be classified under head and neck skin cancer. Metastases to the eyelid are not covered by this staging system.
Eyelid melanomas, which may arise from lesions within the conjunctiva (posterior eyelid lamella) or from lesions within the eyelid skin (anterior eyelid lamella) are not included in this chapter. Please refer to the chapters on conjunctival melanoma or skin melanoma for melanomas affecting the ocular adnexa.
Eyelid Merkel cell carcinoma is not staged using this system but instead is staged using the Merkel cell carcinoma staging system (Chapter 46). We encourage those who care for these patients to work with their registries to collect the ophthalmic items listed under Registry Data Collection Variables in the Merkel cell carcinoma chapter to help inform local control and treatment-related side effects, as well as potential biomarkers for metastatic disease going forward.
| These histopathologic types of cancer… | Are staged according to the classification for… | and can be found in chapter… |
|---|---|---|
| Carcinomas of the head and neck with direct extension to eyelid | Cutaneous carcinoma of the head and neck | 15 |
| Merkel cell carcinoma of the eyelid | Merkel cell carcinoma | 46 |
| Melanoma of the eyelid | Melanoma of the skin | 47 |
Summary of Changes
| Change | Details of Change | Level of Evidence |
|---|---|---|
| Definition of Primary Tumor (T) | T1, T2, T3, and T4 category definitions have been revised based on anatomic extent of primary tumor rather than subjective descriptions, such as “surgical resectability” or “need to do enucleation.” | III |
| Definition of Regional Lymph Node (N) | N1 category has been divided into N1 and N2 based on size and location of positive lymph node(s). | III |
| AJCC Prognostic Stage Groups | Stage groups have been modified to incorporate new T and N categories; Stage III is defined as node-positive disease and Stage IV as distant metastases. | III |
ICD-O-3 Topography Codes
| Code | Description |
|---|---|
| C44.1 | Eyelid |
WHO Classification of Tumors
This list includes histology codes and preferred terms from the WHO Classification of Tumors and the International Classification of Diseases for Oncology (ICD-O). Most of the terms in this list represent malignant behavior. For cancer reporting purposes, behavior codes /3 (denoting malignant neoplasms), /2 (denoting in situ neoplasms), and in some cases /1 (denoting neoplasms with uncertain and unknown behavior) may be appended to the 4-digit histology codes to create a complete morphology code.
| Code | Description |
|---|---|
| 8070 | Squamous cell carcinoma |
| 8090 | Basal cell carcinoma |
| 8140 | Adenocarcinoma, NOS |
| 8200 | Adenoid cystic carcinoma |
| 8390 | Skin appendage carcinoma |
| 8400 | Sweat gland adenocarcinoma |
| 8401 | Apocrine adenocarcinoma |
| 8407 | Sclerosing sweat duct carcinoma |
| 8410 | Sebaceous carcinoma |
| 8413 | Eccrine adenocarcinoma |
| 8430 | Mucoepidermoid carcinoma |
| 8480 | Mucinous adenocarcinoma |
| 8481 | Mucin-producing adenocarcinoma |
| 8940 | Mixed tumor, malignant, NOS |
| 8941 | Carcinoma in pleomorphic adenoma |
| 8980 | Carcinosarcoma, NOS |
Histology is not ideal for clinical use in patient care, as it describes an unspecified or outdated diagnosis. Data collectors may use this code only if there is not enough information in the medical record to document a more specific diagnosis.
LeBoit PE, Burg G, Weedon D, Sarasin A, eds. World Health Organization Classification of Tumours. Pathology and Genetics of Skin Tumours. Lyon: IARC Press; 2006. Used with permission.
International Agency for Research on Cancer, World Health Organization. International Classification of Diseases for Oncology. ICD-O-3-Online.http://codes.iarc.fr/home. Accessed August 16, 2017. Used with permission.
Eyelid carcinomas are the most common malignancies of the eyelid region. A wide variety of carcinomas may involve either the skin or the tarsal and conjunctival layer of the eyelid. Critical size criteria defining the T category for eyelid carcinomas are inherently different from those of other anatomic sites because of the unique anatomic considerations in the eyelid region. In this edition, we further refine the definitions of T and N categories for eyelid carcinoma. Management of eyelid carcinomas consists of surgery in most instances, as well as the judicious use of adjuvant radiation therapy and topical chemotherapy in select patients. In addition, new targeted, systemic treatments aim to preserve the eye and its function in patients with locally advanced disease that previously was treated by orbital exenteration. The functional and anatomic considerations in the eyelid and periocular region make carcinomas of the eyelid unique in terms of AJCC prognostic criteria, outcome reporting, patient selection for clinical trials, and the choice of appropriate treatments.
The TNM classification of eyelid carcinomas reflects both morbidity and mortality risks in order to provide useful guidelines for patient management.1-5 These relate to survival but also to local control as outcome measures. The tumor biology of primary eyelid carcinoma encompasses a broad spectrum of behaviors, from indolent low-grade tumors, such as nodular BCCs, to highly aggressive sebaceous and Merkel cell carcinomas.
Primary eyelid carcinomas mainly include BCCs (90%) which rarely are metastatic but also include other carcinomas with a more pronounced metastatic potential, such as SCC, sebaceous carcinoma, Merkel cell carcinoma, and less common histopathologic types.6-16
Melanomas involving the eyelid are addressed in other chapters (see chapters Conjunctival Melanoma and Melanoma of the Skin).
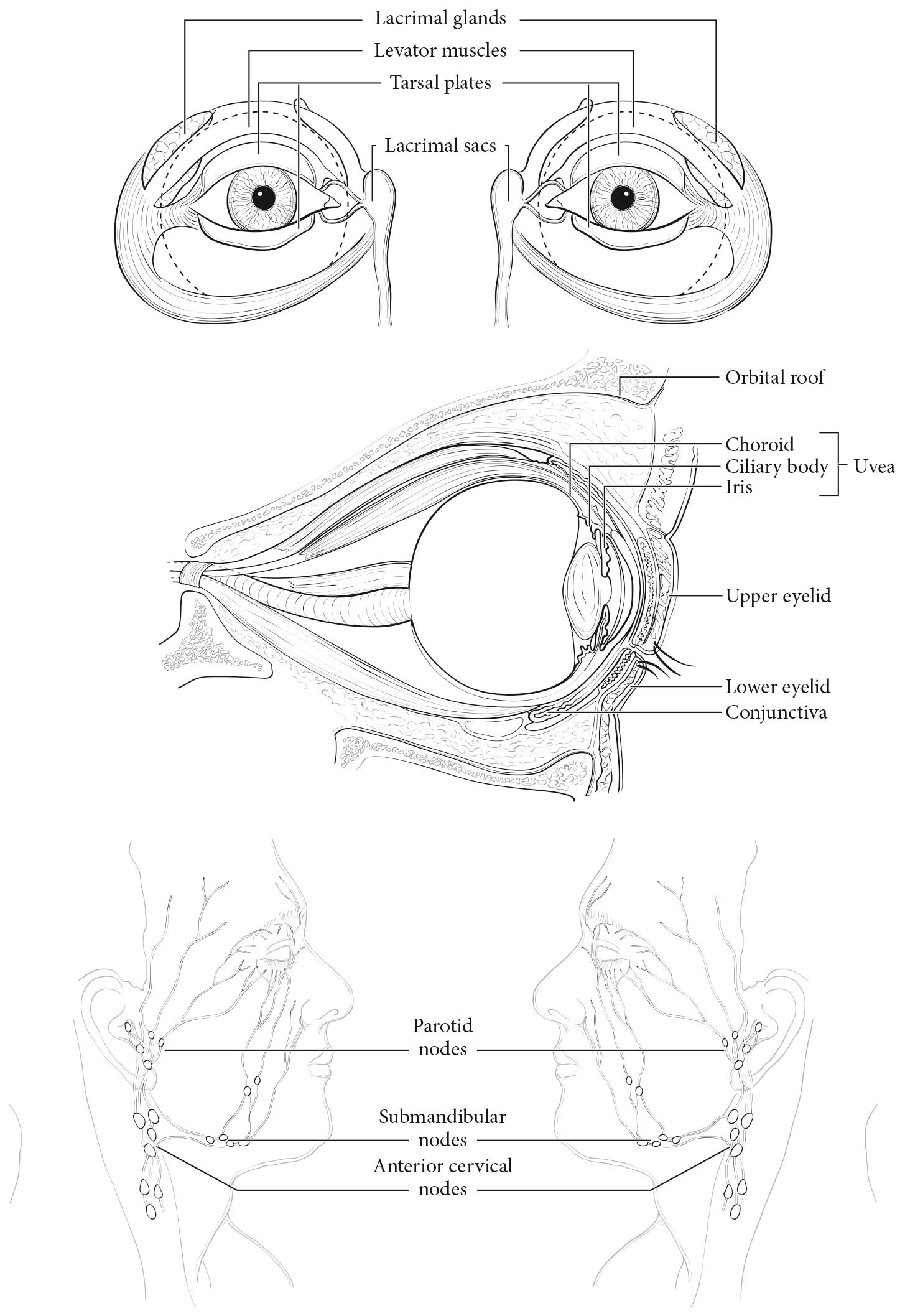
The eyelid is composed of anterior and posterior lamellae, which divide along the mucocutaneous lid margin. From anterior to posterior, the eyelid is composed of skin, orbicularis muscle, tarsus, and conjunctiva. The levator aponeurosis and Müller's muscle are attached at the superior aspect of the tarsus, with analogous retractors in the lower eyelid. There is a rich supply of sebaceous, eccrine, and apocrine sweat glands; accessory lacrimal and neuroendocrine glandular elements are diffused within the eyelid, caruncle, and periorbital tissues. Sebaceous glands are concentrated in the tarsus, in the eyelash margin, and within smaller pilosebaceous units that cover the eyelid and caruncle. Accessory lacrimal glands are located at the upper edge of the tarsus (accessory lacrimal glands of Wolfring) and in the fornix (accessory lacrimal glands of Krause). Glandular elements and skin are the precursor cell types for carcinoma of the eyelid.
The eyelids are supplied with lymphatics that drain into the preauricular, intraparotid, submandibular, and other cervical lymph node basins (Figure 82.1). Recent investigations have shown that all areas of the eyelids may drain into the parotid nodes, in addition to the medial lids draining into the submandibular nodes.12
Staging of eyelid carcinoma begins with a comprehensive ophthalmic, orbital, and periorbital clinical examination. This approach includes a slit lamp or equivalent biomicroscopic evaluation, neuro-ophthalmic examination for evidence of perineural invasion, and regional assessment of the head and neck to include lymphatic drainage basins. Preoperative photography of the extent of disease is recommended.
Carcinoma of the eyelid may extend directly into adjacent structures through mechanisms of direct contiguous invasion, perineural or intravascular spread, and mucosal invasion. Sites of local invasion include the lacrimal drainage system, orbital soft tissue and bone, globe, face, nasal cavity and paranasal sinuses, orbital apex, base of the skull, and central nervous system.
With the exception of BCC, which only rarely metastasizes to the regional lymph nodes, all eyelid carcinomas have the propensity for lymph node metastasis. Historically, it is known that for head and neck squamous carcinomas, lymph node metastasis is a vital independent prognostic factor.13,17
A clinically positive lymph node should be biopsied, and if positive, additional surgery and/or radiation therapy should be offered to achieve regional control.13
The decision to do careful and frequent lymph node evaluation and/or possible biopsy of the draining lymph nodes for eyelid carcinomas should be based on tumor size, histopathologic type, and tumor grade. Analogous to the experience with ocular adnexal melanomas, in the past 15 years, new insights have been gained regarding the value of sentinel lymph node (SLN) biopsy as a staging method for eyelid carcinomas, specifically eyelid Merkel cell and sebaceous carcinomas.18-24
It has been shown that standard clinical and imaging assessment of the regional lymph nodes fails to detect lymph node metastasis in up to 25% of cases of head and neck squamous carcinomas and 32% of head and neck Merkel cell carcinomas. Studies suggest that lymph node dissection in all patients is not justified because of significant morbidity, surgical risk, and low yield for positive nodes. However, SLN biopsy may prove useful for nodal staging, particularly when sampling first-order lymph nodes.22 When positive, SLN biopsy provides critical staging information leading to the selection of patients who may benefit from additional treatments.18,21-23
Technetium-99m lymphoscintigraphy followed by SLN biopsy requires modest adaptation for use in patients with eyelid carcinoma.25,26 The volume of radioactive isotope is reduced to match the reduced thickness and size of the eyelid tissues. Step serial sectioning and immunohistochemical staining improve the sensitivity of this sampling technique.26,27Since the AJCC Cancer Staging Manual, 7th Edition, several manuscripts have attempted to assess the risk of nodal metastasis as a function of AJCC T category for various histologic subtypes of eyelid carcinoma. Recent research suggests that the 7th Edition clinical stage T2b or greater for eyelid sebaceous carcinomas, squamous carcinomas, and Merkel cell carcinomas may be associated with increased risk of nodal metastasis.6,8,14,16,27
Distant metastasis associated with eyelid carcinomas is most likely to occur in very large tumors (T3 or greater) and in the more aggressive histologies, such as Merkel cell carcinoma, sebaceous carcinoma, and microcystic adnexal carcinoma.14,28,29
Imaging
The requirement for imaging modalities, including computed tomography (CT), magnetic resonance (MR) imaging, and ultrasonography, is highly dependent on the histopathologic type of eyelid carcinoma and clinical extent of the primary eyelid tumor.
For locally advanced eyelid carcinomas, an orbital CT scan with axial and coronal views with contrast, with both tissue and bone window settings, should be obtained initially to evaluate the extent of tumor into the orbital soft tissue or periorbital structures, such as the paranasal sinuses or nasal cavity, or posteriorly or superiorly into the skull base.
For the more aggressive tumor types with the potential for lymph node metastasis, such as sebaceous carcinomas and squamous carcinomas of the eyelid that are >=T2b, a baseline imaging study of the head and neck should be obtained. This study might be a CT scan with axial and coronal cuts to include the regional lymph nodes. Ultrasonography of the regional lymph nodes also is quite good at detecting abnormal lymph nodes that may then be biopsied with fine-needle aspiration. SLN biopsy should be considered only in patients who have had negative findings on clinical examination and on imaging studies such as CT and ultrasound.25,26,29
MR imaging with gadolinium enhancement is the imaging study of choice if overt clinically symptomatic invasion of large nerves is suspected in association with a previously treated or recurrent locally advanced eyelid carcinoma. If metastatic spread is suspected, as in the case of a large eyelid Merkel cell carcinoma, a positron emission tomography (PET)/CT scan may be helpful in evaluating for widespread metastatic disease and for response to treatment.
Precise macroscopic description is essential: the surgical nature of the excisional surgical specimen (i.e., excisional biopsy, wide local excision, or radical excision including exenteration), as well as its size, should be noted. Incisional biopsies performed to establish the pathological diagnosis are considered part of the clinical classification. The specimen should be oriented carefully and inked for margin evaluation. Pathological classification is based on the specific tumor type, its differentiation (grade), and the completeness of tumor removal. Greatest tumor dimension and evaluation of the surgical specimen margins are mandatory.
Prognostic Factors Required for Stage Grouping
Beyond the factors used to assign T, N, or M categories, no additional prognostic factors are required for stage grouping.
Additional Factors Recommended for Clinical Care
The diagnosis of sebaceous carcinoma should prompt consideration of a workup to exclude Muir-Torre syndrome, a phenotypic variant of hereditary nonpolyposis colon cancer, or Lynch syndrome. Sebaceous neoplasia (including adenoma, epithelioma, and carcinoma) and keratoacanthomas are cutaneous manifestations of Muir-Torre syndrome, together with visceral malignancies, especially colorectal and endometrial carcinomas. The disorder has been linked to mutations in MLH1 and MSH2.30-33
Defective mismatch repair is important for detection of Lynch syndrome and, accordingly, is a feature of tumors arising in Muir-Torre syndrome.30-32 Tumor DNA may be tested for microsatellite instability by polymerase chain reaction technology using a panel of at least five microsatellite markers assessing for changes in the length of the microsatellite loci. In addition, immunohistochemistry may be performed for parallel assessment for retained expression of mismatch repair proteins (MLH1, MSH2, MSH6, PMS2) in formalin-fixed, paraffin-embedded tissue. Intact expression of all four proteins indicates that mismatch repair enzymes are intact but does not entirely exclude Lynch syndrome, as missense mutations may lead to a nonfunctional protein with retained immunogenicity.
The authors have not noted any emerging factors for clinical care.
The AJCC recently established guidelines that will be used to evaluate published statistical prediction models for the purpose of granting endorsement for clinical use.34 Although this is a monumental step toward the goal of precision medicine, this work was published only very recently. Therefore, the existing models that have been published or may be in clinical use have not yet been evaluated for this cancer site by the Precision Medicine Core of the AJCC. In the future, the statistical prediction models for this cancer site will be evaluated, and those that meet all AJCC criteria will be endorsed.
The following stratification criteria are recommended for clinical trials for various eyelid carcinomas:
Definition of Primary Tumor (T)
| T Category | T Criteria |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor less than or equal to 10 mm in greatest dimension |
| T1a | Tumor does not invade the tarsal plate or eyelid margin |
| T1b | Tumor invades the tarsal plate or eyelid margin |
| T1c | Tumor involves full thickness of the eyelid |
| T2 | Tumor greater than 10 mm but less than or equal to 20 mm in greatest dimension |
| T2a | Tumor does not invade the tarsal plate or eyelid margin |
| T2b | Tumor invades the tarsal plate or eyelid margin |
| T2c | Tumor involves full thickness of the eyelid |
| T3 | Tumor greater than 20 mm but less than or equal to 30 mm in greatest dimension |
| T3a | Tumor does not invade the tarsal plate or eyelid margin |
| T3b | Tumor invades the tarsal plate or eyelid margin |
| T3c | Tumor involves full thickness of the eyelid |
| T4 | Any eyelid tumor that invades adjacent ocular, orbital, or facial structures |
| T4a | Tumor invades ocular or intraorbital structures |
| T4b | Tumor invades (or erodes through) the bony walls of the orbit or extends to the paranasal sinuses or invades the lacrimal sac/nasolacrimal duct or brain |
Definition of Regional Lymph Node (N)
| N Category | N Criteria |
|---|---|
| NX | Regional lymph nodes cannot be assessed |
| N0 | No evidence of lymph node involvement |
| N1 | Metastasis in a single ipsilateral regional lymph node, less than or equal to 3 cm in greatest dimension |
| N1a | Metastasis in a single ipsilateral lymph node based on clinical evaluation or imaging findings |
| N1b | Metastasis in a single ipsilateral lymph node based on lymph node biopsy |
| N2 | Metastasis in a single ipsilateral lymph node, greater than 3 cm in greatest dimension, or in bilateral or contralateral lymph nodes |
| N2a | Metastasis documented based on clinical evaluation or imaging findings |
| N2b | Metastasis documented based on microscopic findings on lymph node biopsy |
Definition of Distant Metastasis (M)
| M Category | M Criteria |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis |
| When T is… | and N is… | and M is… | Then the stage group is… |
|---|---|---|---|
| Tis | N0 | M0 | 0 |
| T1 | N0 | M0 | IA |
| T2a | N0 | M0 | IB |
| T2b-c, T3 | N0 | M0 | IIA |
| T4 | N0 | M0 | IIB |
| Any T | N1 | M0 | IIIA |
| Any T | N2 | M0 | IIIB |
| Any T | Any N | M1 | IV |
HISTOLOGIC GRADE (G)
A histologic grading system is used predominantly for SCCs and sebaceous carcinomas. It is not used for Merkel cell carcinoma or BCC.
| G | G Definition |
|---|---|
| GX | Grade cannot be assessed |
| G1 | Well differentiated |
| G2 | Moderately differentiated |
| G3 | Poorly differentiated |
| G4 | Undifferentiated |