Introduction
- Pharmacology. Digoxin-specific antibodies are produced in immunized sheep and have a high binding affinity for digoxin and, to a lesser extent, digitoxin and other cardiac glycosides. The Fab fragments used to treat poisoning are derived by cleaving the whole antibodies. Once the digoxin-Fab complex is formed, the digoxin molecule is no longer pharmacologically active. The complex enters the circulation, is renally eliminated and cleared by the reticuloendothelial system, and has a half-life of 15-20 hours (may increase 10-fold with renal impairment). Reversal of signs of digitalis intoxication usually occurs within 30-60 minutes of administration (average initial response, 19 minutes), with complete reversal varying up to 24 hours (average, 88 minutes).
- Indications. Digoxin-specific antibodies are used for life-threatening arrhythmias, hyperkalemia (≥5 mEq/L), or hemodynamic instability caused by acute and chronic digoxin intoxication. Treatment should be based on elevated levels that are at steady state (or are post-distributional) as well as the presence of significant symptoms (eg, hyperkalemia, ventricular arrhythmias, bradyarrhythmias, and hypotension). Note: digoxin-specific Fab fragments can also bind with varying affinity to other cardiac glycosides, including digitoxin, ouabain, oleander glycosides, and possibly glycosides in lily of the valley, Strophanthus, squill, and toad venom (Bufo species cardenolides).
- Contraindications. There is no known contraindication. Use caution in patients with sensitivity to ovine (sheep) products; a skin test for hypersensitivity may be performed in such patients, with the use of diluted reconstituted drug. There are no reports of hypersensitivity reactions in patients who have received the drug more than once (although this is a theoretical risk). Product may contain traces of papain; therefore, caution is advised in patients with allergies to papain, chymopapain, papaya extracts, and the pineapple enzyme bromelain.
- Adverse effects
- Monitor the patient for potential hypersensitivity reactions and serum sickness. A dose- and rate-related (anaphylactoid) reaction may occur with rapid IV administration.
- In patients with renal insufficiency and impaired clearance of the digitalis-Fab complex, a delayed rebound of free serum digoxin levels may occur for up to 130 hours.
- Removal of the inotropic effect of digitalis may exacerbate preexisting heart failure.
- With removal of the digitalis effect, patients with preexisting atrial fibrillation may develop an accelerated ventricular response.
- Removal of the digitalis effect may reactivate sodium-potassium-ATPase and shift potassium into cells, causing a drop in the serum potassium level.
- Use in pregnancy. FDA Category C (indeterminate). This does not preclude its acute, short-term use for a seriously symptomatic patient (Introduction).
- Drug or laboratory interactions. The digoxin-Fab complex cross-reacts with the antibody commonly used in quantitative immunoassay techniques. This results in falsely high serum concentrations of digoxin owing to measurement of the inactive Fab complex (total serum digoxin levels may increase 10- to 21-fold). However, some assays and procedures may measure free digoxin levels, which may be useful for patients with renal impairment (to monitor a rebound in free serum digoxin levels after administration of Fab fragments).
- Dosage and method of administration. Each vial of either digoxin-immune Fab product binds 0.5 mg of digoxin.
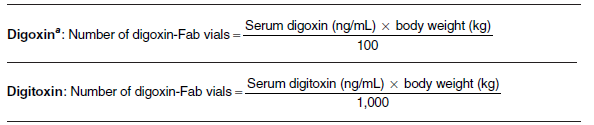
- Complete neutralization/equimolar dosing; known level or amount ingested. Estimation of the dose of Fab is based on the body burden of digitalis. This may be calculated if the approximate amount ingested is known (Table III-8) or if the steady-state (post-distributional) serum drug concentration is known (Table III-9). The steady-state serum drug concentration should be determined at least 12-16 hours after the last dose. Note: Use of the ingested digoxin dose calculation will generally overestimate the Fab dose requirement. Also, calculation of the digoxin body burden is based on an estimated volume of distribution of 5-6 L/kg; however, the Vd may be as high as 10 L/kg. If the patient fails to respond to the initial treatment, the dose may have to be increased by an additional 50%.
- Empiric dosing (unknown level and severe toxicity). If the amount ingested or the post-distributional level is not known and the patient has life-threatening dysrhythmias, use empiric dosing. The manufacturer recommends that 20 (10 for children) and 6 vials be given empirically for acute and chronic overdoses, respectively. However, average dose requirements are 10 vials for acute and 1-3 vials for chronic digoxin intoxication.
- Titration dosing. Theoretically, Fab may be used to neutralize a portion of the digoxin body burden to reverse toxicity but maintain therapeutic benefits. Many patients will respond to one-half or less of the calculated neutralizing dose based on body burden. The Fab dose can be estimated by subtracting the desired digoxin level from the measured post-distributional level before the calculation is completed. Alternately, if the patient is hemodynamically stable, the drug can be given empirically, 1-2 vials at a time, with titration to clinical effect. A proposed strategy has been to infuse the initial or loading dose over 30-60 minutes and then allow 1 hour after the end of the infusion period to assess the need for additional doses. This may optimize binding and reduce antidote waste. However, partial dosing has been associated with recurrences of symptoms in some digoxin-poisoned patients.
- Reconstitute the drug with 4 mL of Sterile Water for Injection USP and administer intravenously over at least 30 minutes. The reconstituted product may be added to 0.9% sodium chloride. Note: Longer infusion periods (1-7 hours) or constant infusions have been suggested to optimize binding of digoxin to the antibodies. The drug may also be given as a rapid bolus for immediately life-threatening arrhythmias.
TABLE III-8. APPROXIMATE DIGOXIN-FAB DOSE IF AMOUNT INGESTED IS KNOWN| Tablets Ingested (0.125-mg Size) | Tablets Ingested (0.25-mg Size) | Approximate Dose Absorbed (mg) | Recommended Dose (No. of Vials) |
|---|
| 5 | 2.5 | 0.5 | 1 |
| 10 | 5 | 1 | 2 |
| 20 | 10 | 2 | 4 |
| 50 | 25 | 5 | 10 |
| 100 | 50 | 10 | 20 |