AUTHOR: Brian Block, MD


Definition
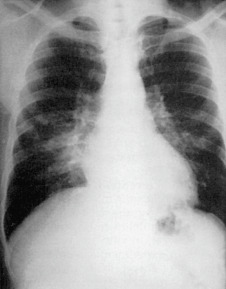
Mycoplasma pneumonia is an infection of the lung parenchyma caused by a small rod-shaped bacterium, Mycoplasma pneumoniae.
Epidemiology & Demographics
Incidence (in U.S.)
- Frequent cause of community-acquired pneumonia (CAP); particularly in children and adults <40 yr
- Causes periodic outbreaks with high secondary attack rate among household contacts because it is easily transmitted1
- Many cases probably resolve without coming to medical attention2
- Asymptomatic carriage thought to be common
Physical Findings & Clinical Presentation
- Common symptoms include fever, cough, headache, and otalgia
- Exam findings include rhonchi or rales, conjunctivitis, lymphadenopathy
- Rash occurs in 10% to 25% of infected individuals, ranging from self-limited morbilliform eruptions to life-threatening rashes including Stevens-Johnson syndrome4
- Some patients develop autoimmune hemolytic anemia due to autoantibodies (cold agglutinins)
- Neurologic manifestations are also possible but less common (mono- or polyneuritis, transverse myelitis, cranial nerve palsies)
- Table E1 summarizes the clinical manifestations of Mycoplasma pneumoniae