Enthesitis related arthritis (ERA) is a subtype of juvenile idiopathic arthritis (JIA) and is associated with the HLA B27 antigen. The International League of Associations for Rheumatology (ILAR) defines ERA using the following criteria: (1) Any patient with both arthritis and enthesitis; (2) the presence of arthritis or enthesitis with two of the following features: Sacroiliac joint tenderness, inflammatory spinal pain, or both; HLA B27 family history in 1st degree relative of medically confirmed HLA B27-associated disease; acute anterior uveitis; onset of arthritis in a boy after the age of 6 yr. Of note, patients with psoriasis or with psoriasis in a 1st degree relative are also excluded.
Juvenile enthesitis-related arthritis
Enthesitis related arthritis, juvenile
| ||||||||
- The most common presenting symptoms of ERA include arthritis, enthesitis, and symptomatic uveitis.
- With the exception of the hip and sacroiliac joints, a majority of the observed arthritis is peripheral. The most common joints to be affected include the ankles, knees, and hips.
- The observed arthritis is typically asymmetric and typically effects fewer than 4 joints.
- While pain and inflammation about the bones of the midfoot are less common, such symptoms are highly suggestive of the disease.
- As the disease process progresses many patients go on to develop clinical and radiologic evidence of spinal and sacroiliac joint involvement.
- Enthesitis is typically asymmetric and more frequently occurs in the lower extremities.
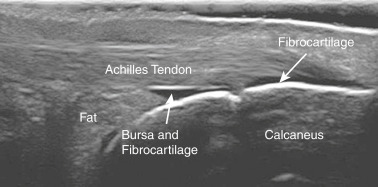
- Enthesitis most frequently occurs at inferior pole of the patella, the plantar fascia insertion at the calcaneus, and finally the Achilles tendon insertion at the calcaneus. More chronic enthesitis may demonstrate evidence of erosion, calcifications, and heterotopic bone formation on radiographs.
- The anterior uveitis observed with ERA is typically acute in onset and manifests with conjunctival injection, pain, and light sensitivity.