AUTHOR: Fred F. Ferri, MD




Definition
Prolactinomas are monoclonal tumors that secrete prolactin.
| ||||||||||||
Epidemiology & Demographics
Incidence
Most common pituitary tumor; nearly 30% of all pituitary adenomas secrete enough prolactin to cause hyperprolactinemia.
Physical Findings & Clinical Presentation
- Men: Decreased facial and body hair, infertility, small testicles; may also have de creased libido, erectile dysfunction, and delayed puberty (caused by decreased testosterone as a result of inhibition of gonadotropin secretion).
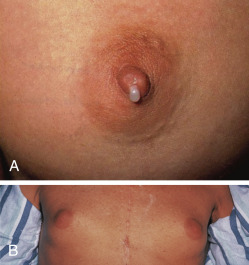
- Women: Physical examination may be normal; history may reveal amenorrhea, galactorrhea (Fig. E1), oligomenorrhea, and anovulation.
- Both sexes: Visual field defects and headache may occur depending on size of tumor and its expansion.