AUTHOR: Corey Elam Goldsmith, MD, FAAN

Definition
Optic neuritis is an inflammation of the optic nerve(s) resulting in impaired visual function and often retroorbital pain worse with eye movements.
Epidemiology & Demographics
Incidence (In U.S.)
1 to 5/100,000 person(s) per year; rates vary according to incidence of multiple sclerosis (MS). Optic neuritis affects 1% to 5% of patients with neurosarcoidosis.
Physical Findings & Clinical Presentation
- Presentation with acute (days) or subacute (weeks) vision loss, often accompanied by retroorbital pain that worsens with eye movements. Visual field defects commonly are present; they can be either diffuse or discrete scotomas and are nonspecific. Fundus examination shows mild disc edema in approximately one third of affected eyes, which is typically less prominent than the disc swelling associated with papilledema (Fig. E1). In the majority of patients, the fundus appearance is normal.
- Marcus Gunn pupil (relative afferent pupillary defect [RAPD]): Consensual response is normal; however, when the flashlight is swung from the unaffected eye to the affected eye, the affected eye’s pupil paradoxically dilates in response to direct light.
- Decreased visual acuity.
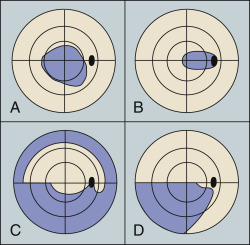
- Unilateral (or bilateral with some diseases) visual field abnormalities-often a central scotoma (Fig. E2) or diffuse (in MS), or altitudinal (in NMOSD).
- Color desaturation; red is most often affected.
- Normal fundus examination in 66% of cases; disc edema is noted in 33% (more frequent and severe when associated with MOGAD, infectious, or granulomatous causes). Other abnormalities can include uveitis, periphlebitis, episcleritis, and retinitis. In neurosarcoidosis, the optic nerve head may exhibit a lumpy appearance suggestive of granulomatous infiltration, and there may be associated vitreitis (Fig. E3).
- May have movement or light induced phosphenes (flashes of light lasting 1 to 2 sec).
- Uhthoff phenomenon (benign exercise- or heat-induced deterioration of vision due to elevated core body temperature, lasting less than 24 h) is seen in some. Vision may also worsen in bright sunlight.
- Over time, the optic disc may atrophy and become pale.
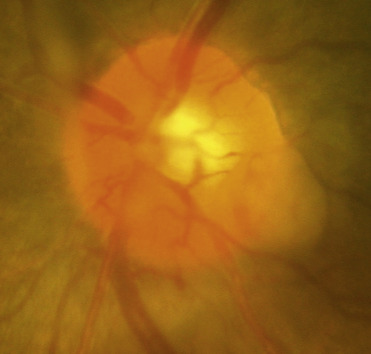
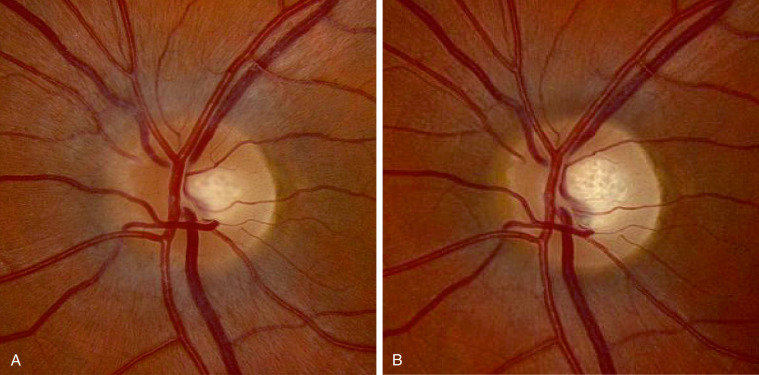
Figure E1 (A) Fundus Photograph of the Left Eye in a Patient with Acute Left Optic Neuritis
Note Mild Nerve Fiber Layer Edema, Greatest at the Nasal Portion of the Disc, Without Hemorrhages or Cotton-Wool Spots. (B) Fundus Photograph of the Left Eye from the Same Patient Taken 3 Mo after Initial Presentation. Note Resolution of Edema and Presence of Mild Temporal Pallor.
From Jankovic J et al: Bradley and Daroff’s neurology in clinical practice, ed 8, Philadelphia, 2022, Elsevier.