Critical
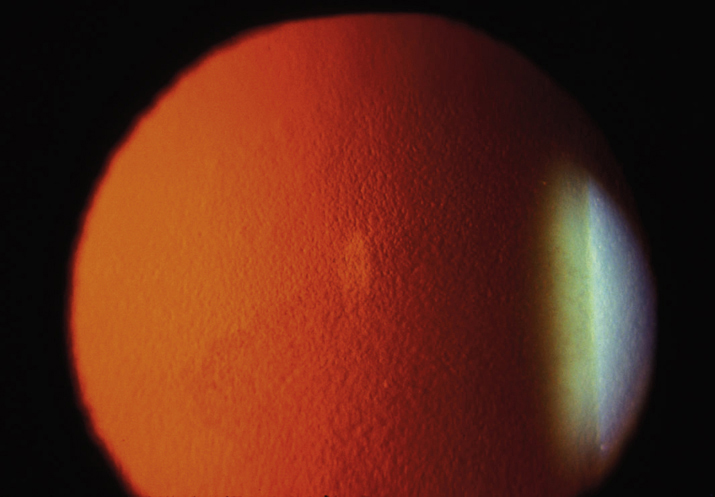
Cornea guttae with stromal +/- epithelial edema (see Figure 4.26.1). Bilateral, but may be asymmetric.
 NOTE: NOTE: | |
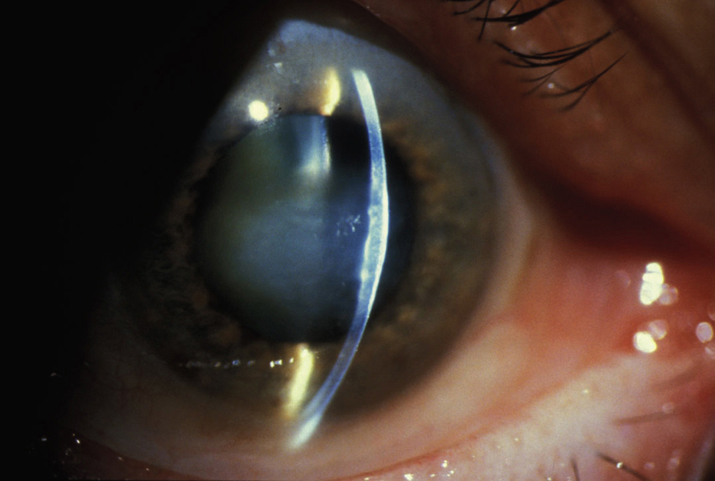
Central cornea guttae without stromal edema is called endothelial dystrophy (see Figure 4.26.2). This condition may progress to Fuchs dystrophy over years. |
Other
Fine pigment dusting on the endothelium, central epithelial edema and bullae, folds in Descemet membrane, stromal edema, subepithelial haze, or scarring.