(See Figure 9.5.1.)
Critical
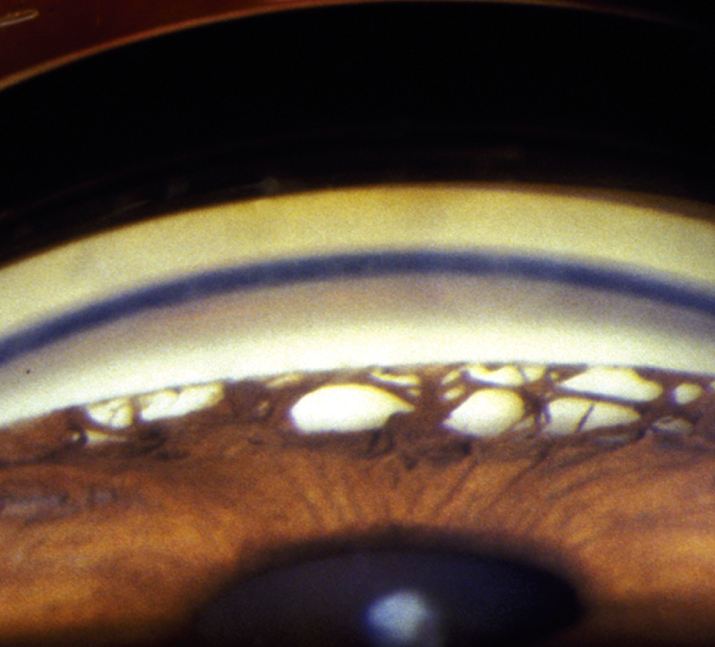
Gonioscopy reveals broad bands of PAS in the angle. The PAS block visualization of the underlying angle structures. Glaucomatous optic nerve and visual field defects.
Other
Elevated IOP.
Usually asymptomatic, although patients with advanced disease may present with decreased vision or visual field loss. Intermittent eye pain, headaches, and blurry vision may occur.
(See Figure 9.5.1.)
Critical
Gonioscopy reveals broad bands of PAS in the angle. The PAS block visualization of the underlying angle structures. Glaucomatous optic nerve and visual field defects.
Other
Elevated IOP.
Gradual narrowing of the angle with prolonged appositional closure.
Prolonged acute angle closure glaucoma or multiple episodes of subclinical attacks of acute angle closure.
Previous flat anterior chamber from surgery, trauma, or hypotony that resulted in the development of PAS.
 NOTE: NOTE: |
While acute angle closure is less common in those of African descent, chronic angle closure is more commonly seen in these patients. |
See 9.1, PRIMARY OPEN-ANGLE GLAUCOMA.