Many are asymptomatic, but patients may report decreased vision depending on the stage.
(See Figure 8.3.1.)
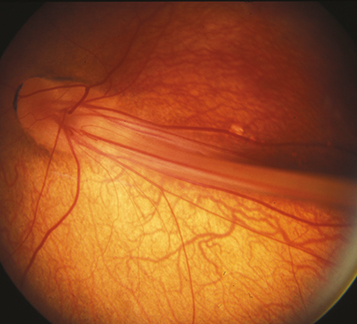
Figure 8.3.1: Familial exudative vitreoretinopathy with a falciform fold.
Critical
Vascular dragging and peripheral retinal nonperfusion, most prominently temporally, although can extend 360 degrees. Bilateral but often asymmetric. Peripheral retinal vessels have a fimbriated border. Present at birth.
Other
Peripheral neovascularization and/or fibrovascular proliferation at the border of vascular and avascular retina; temporal dragging of macula through contraction of fibrovascular tissue; radial retinal folds; vitreous hemorrhage; epiretinal membranes; tractional, exudative, and/or rhegmatogenous retinal detachment; peripheral intraretinal and subretinal lipid exudation. May present with strabismus or leukocoria in childhood. Cataract, band keratopathy, neovascular glaucoma, or phthisis possible.
Due to defects in the Wnt signaling pathway. Often autosomal dominant, but can be autosomal recessive or X-linked. Usually no history of prematurity or oxygen therapy (differentiates it from ROP).
Laser of peripheral avascular retina is performed if there is neovascularization and/or exudation. Scleral buckling or vitrectomy can be considered for retinal detachments. Anti-VEGF treatment may be effective in cases with neovascularization, though further long-term studies are needed. Treat amblyopia as needed. Genetic testing and examination of family members recommended.
FEVR is a lifelong disease. All patients should be followed throughout life to monitor for progression.